

Diagnostic Stewardship in Community-Acquired Pneumonia With Syndromic Molecular Testing: A Randomized Clinical Trial
- PMID: 38446481
- PMCID: PMC10918504
- DOI: 10.1001/jamanetworkopen.2024.0830
Diagnostic Stewardship in Community-Acquired Pneumonia With Syndromic Molecular Testing: A Randomized Clinical Trial
Erratum in
-
Error in Figure 1.JAMA Netw Open. 2025 Apr 1;8(4):e258665. doi: 10.1001/jamanetworkopen.2025.8665. JAMA Netw Open. 2025. PMID: 40168029 Free PMC article. No abstract available.
Abstract
Importance: Lower respiratory tract (LRT) infections, including community-acquired pneumonia (CAP), are a leading cause of hospital admissions and mortality. Molecular tests have the potential to optimize treatment decisions and management of CAP, but limited evidence exists to support their routine use.
Objective: To determine whether the judicious use of a syndromic polymerase chain reaction (PCR)-based panel for rapid testing of CAP in the emergency department (ED) leads to faster, more accurate microbiological test result-based treatment.
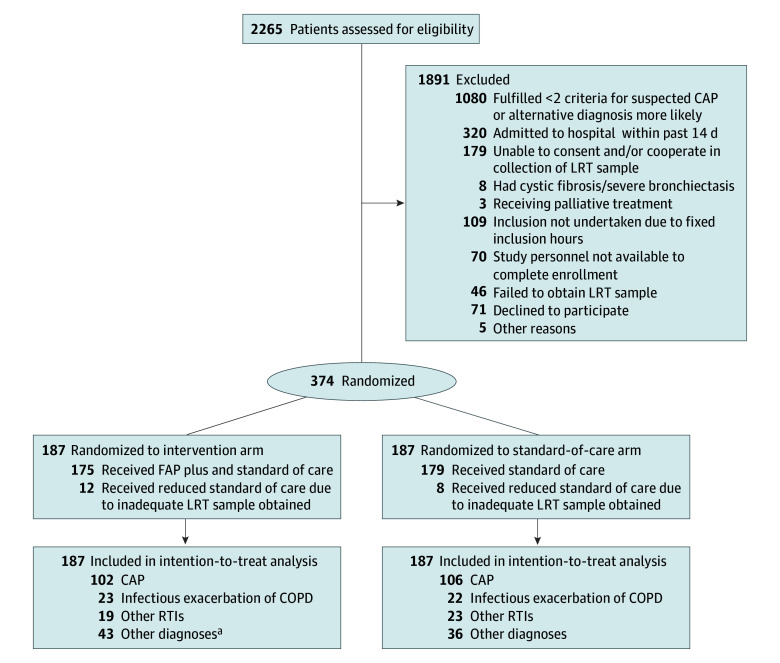
Design, setting, and participants: This parallel-arm, single-blinded, single-center, randomized clinical superiority trial was conducted between September 25, 2020, and June 21, 2022, in the ED of Haukeland University Hospital, a large tertiary care hospital in Bergen, Norway. Adult patients who presented to the ED with suspected CAP were recruited. Participants were randomized 1:1 to either the intervention arm or standard-of-care arm. The primary outcomes were analyzed according to the intention-to-treat principle.
Intervention: Patients randomized to the intervention arm received rapid syndromic PCR testing (BioFire FilmArray Pneumonia plus Panel; bioMérieux) of LRT samples and standard of care. Patients randomized to the standard-of-care arm received standard microbiological diagnostics alone.
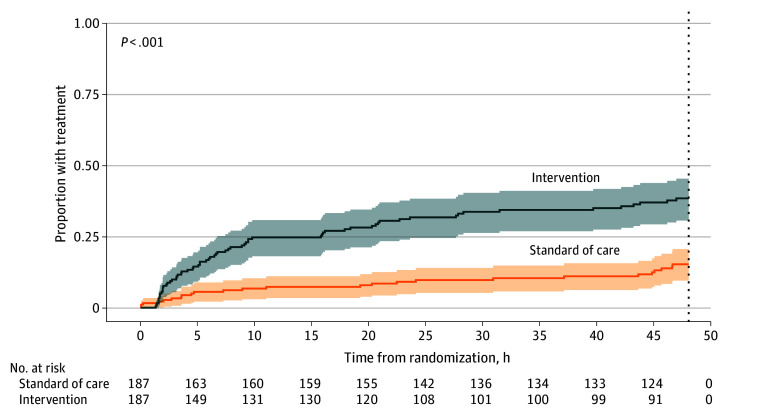
Main outcomes and measures: The 2 primary outcomes were the provision of pathogen-directed treatment based on a microbiological test result and the time to provision of pathogen-directed treatment (within 48 hours after randomization).
Results: There were 374 patients (221 males [59.1%]; median (IQR) age, 72 [60-79] years) included in the trial, with 187 in each treatment arm. Analysis of primary outcomes showed that 66 patients (35.3%) in the intervention arm and 25 (13.4%) in the standard-of-care arm received pathogen-directed treatment, corresponding to a reduction in absolute risk of 21.9 (95% CI, 13.5-30.3) percentage points and an odds ratio for the intervention arm of 3.53 (95% CI, 2.13-6.02; P < .001). The median (IQR) time to provision of pathogen-directed treatment within 48 hours was 34.5 (31.6-37.3) hours in the intervention arm and 43.8 (42.0-45.6) hours in the standard-of-care arm (mean difference, -9.4 hours; 95% CI, -12.7 to -6.0 hours; P < .001). The corresponding hazard ratio for intervention compared with standard of care was 3.08 (95% CI, 1.95-4.89). Findings remained significant after adjustment for season.
Conclusions and relevance: Results of this randomized clinical trial indicated that routine deployment of PCR testing for LRT pathogens led to faster and more targeted microbial treatment for patients with suspected CAP. Rapid molecular testing could complement or replace selected standard, time-consuming, laboratory-based diagnostics.
Trial registration: ClinicalTrials.gov Identifier: NCT04660084.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
