

Management for degenerative lumbar spondylolisthesis: a network meta-analysis and systematic review basing on randomized controlled trials
- PMID: 38446872
- PMCID: PMC11093486
- DOI: 10.1097/JS9.0000000000001228
Management for degenerative lumbar spondylolisthesis: a network meta-analysis and systematic review basing on randomized controlled trials
Erratum in
-
Management for degenerative lumbar spondylolisthesis: a network meta-analysis and systematic review basing on randomized controlled trials: Erratum.Int J Surg. 2024 Jul 1;110(7):4530. doi: 10.1097/JS9.0000000000001929. Int J Surg. 2024. PMID: 39042081 Free PMC article. No abstract available.
Abstract
Background: Consensus on the various interventions for degenerative lumbar spondylolisthesis (DLS) remains unclear.
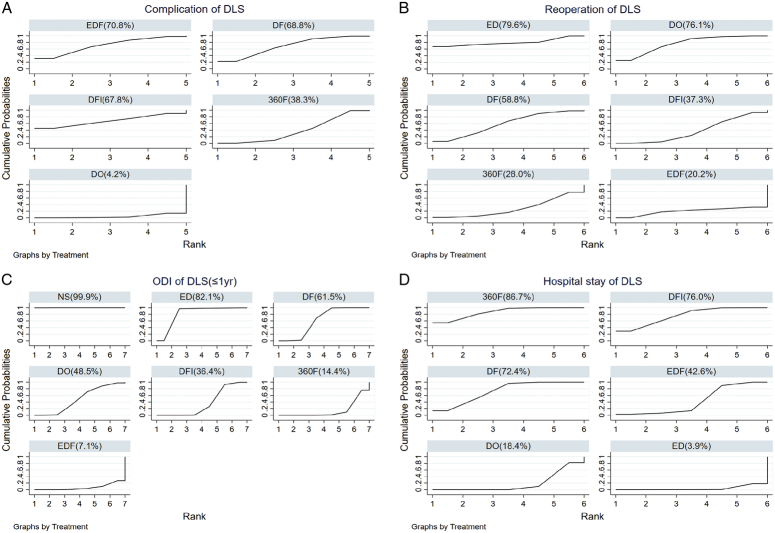
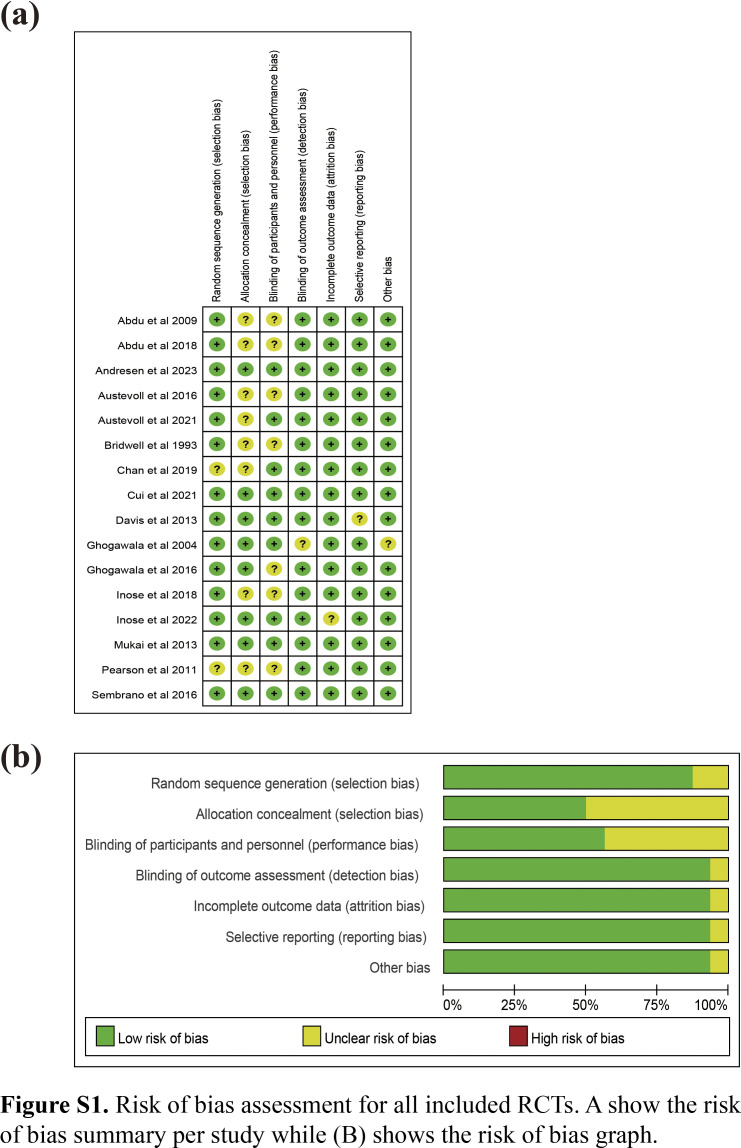
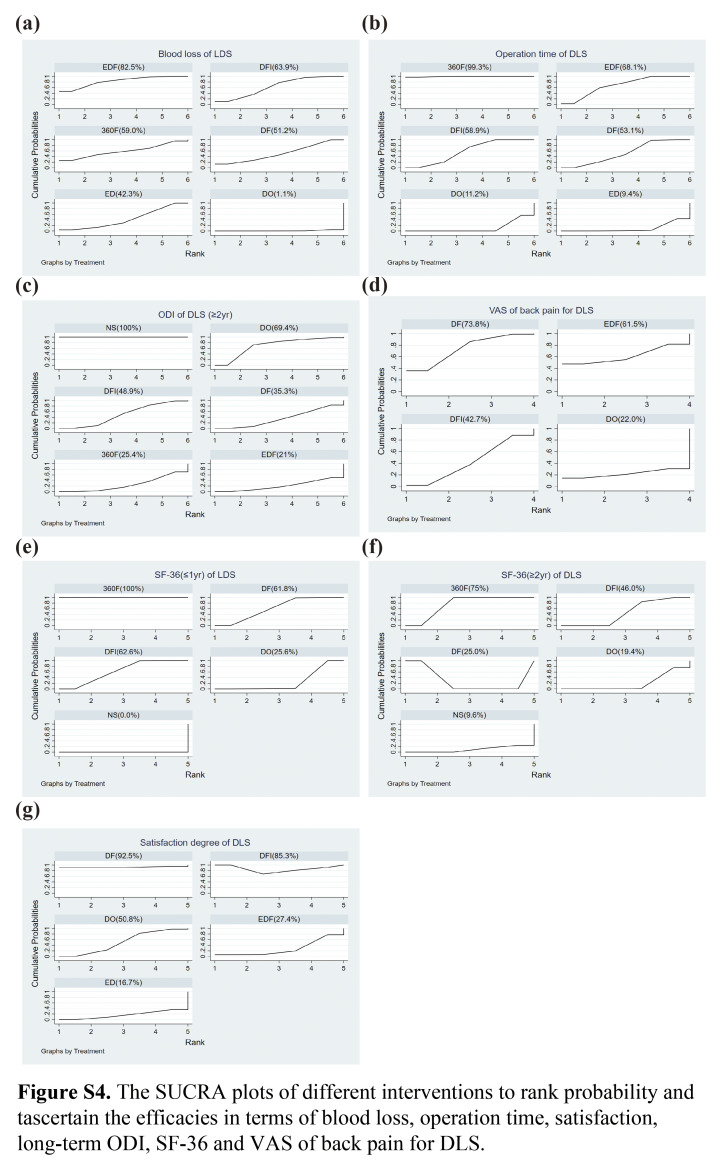
Materials and methods: The authors searched PubMed, Embase, Cochrane Library, Web of Science, and major scientific websites until 01 November 2023, to screen eligible randomized controlled trials (RCTs) involving the treatment of DLS. The seven most common DLS interventions [nonsurgical (NS), decompression only (DO), decompression plus fusion without internal fixation (DF), decompression plus fusion with internal fixation (DFI), endoscopic decompression plus fusion (EDF), endoscopic decompression (ED), and circumferential fusion (360F)] were compared. The primary (pain and disability) and secondary (complications, reoperation rate, operation time, blood loss, length of hospital stay, and satisfaction) outcomes were analyzed.
Results: Data involving 3273 patients in 16 RCTs comparing the efficacy of different interventions for DLS were reported. In terms of improving patient pain and dysfunction, there was a significant difference between surgical and NS. EDF showed the greatest improvement in short-term and long-term dysfunction (probability, 7.1 and 21.0%). Moreover, EDF had a higher complication rate (probability 70.8%), lower reoperation rate (probability, 20.2%), and caused greater blood loss (probability, 82.5%) than other surgical interventions. Endoscopic surgery had the shortest hospitalization time (EDF: probability, 42.6%; ED: probability, 3.9%). DF and DFI had the highest satisfaction scores.
Conclusions: Despite the high complication rate of EDF, its advantages include improvement in pain, lower reoperation rate, and shorter hospitalization duration. Therefore, EDF may be a good option for patients with DLS as a less invasive surgical approach.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest for this work.
Figures










References
-
- Fitzgerald JA, Newman PH. Degenerative spondylolisthesis. J Bone Joint Surg Br 1976;58:184–192. - PubMed
-
- Gadjradj PS, Basilious M, Goldberg JL, et al. Decompression alone versus decompression with fusion in patients with lumbar spinal stenosis with degenerative spondylolisthesis: a systematic review and meta-analysis. Eur Spine J 2023;32:1054–1067. - PubMed
-
- Sengupta DK, Herkowitz HN. Degenerative spondylolisthesis: review of current trends and controversies. Spine 2005;30(6 Suppl):S71–S81. - PubMed
-
- Iguchi T, Wakami T, Kurihara A, et al. Lumbar multilevel degenerative spondylolisthesis: radiological evaluation and factors related to anterolisthesis and retrolisthesis. J Spinal Disord Tech 2002;15:93–99. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
