

A 14-gene B-cell immune signature in early-stage triple-negative breast cancer (TNBC): a pooled analysis of seven studies
- PMID: 38447275
- PMCID: PMC10924177
- DOI: 10.1016/j.ebiom.2024.105043
A 14-gene B-cell immune signature in early-stage triple-negative breast cancer (TNBC): a pooled analysis of seven studies
Abstract
Background: Early-stage triple-negative breast cancer (TNBC) displays clinical and biological diversity. From a biological standpoint, immune infiltration plays a crucial role in TNBC prognosis. Currently, there is a lack of genomic tools aiding in treatment decisions for TNBC. This study aims to assess the effectiveness of a B-cell/immunoglobulin signature (IGG) alone, or in combination with tumor burden, in predicting prognosis and treatment response in patients with TNBC.
Methods: Genomic and clinical data were retrieved from 7 cohorts: SCAN-B (N = 874), BrighTNess (n = 482), CALGB-40603 (n = 389), METABRIC (n = 267), TCGA (n = 118), GSE58812 (n = 107), GSE21653 (n = 67). IGG and a risk score integrating IGG with tumor/nodal staging (IGG-Clin) were assessed for event-free survival (EFS) and overall survival (OS) in each cohort. Random effects model was used to derive pooled effect sizes. Association of IGG with pathological complete response (pCR) was assessed in CALGB-40603 and BrighTNess. Immune significance of IGG was estimated through CIBERSORTx and EcoTyper.
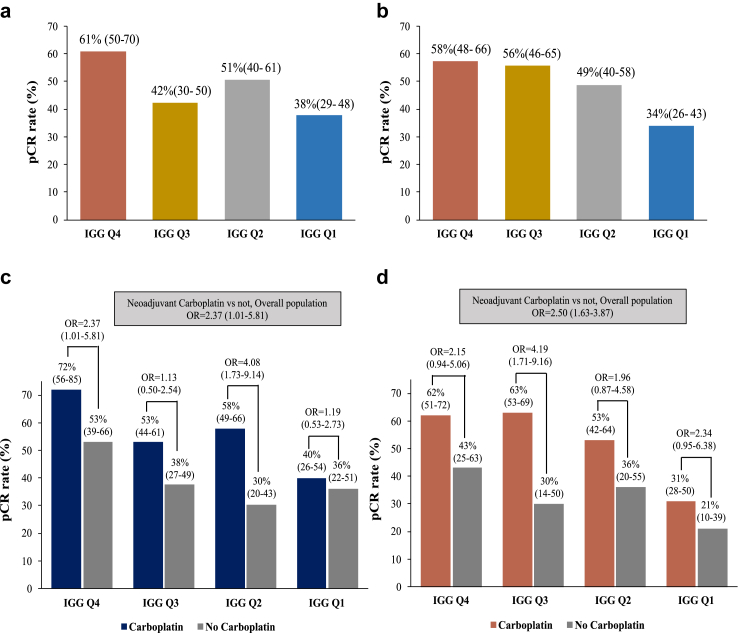
Findings: IGG was associated with improved EFS (pooled HR = 0.77, [95% CI = 0.70-0.85], I2 = 18%) and OS (pooled HR = 0.79, [0.73-0.85], I2 = 0%) across cohorts, and was predictive of pCR in CALGB-40603 (OR 1.25, [1.10-1.50]) and BrighTNess (OR 1.57 [1.25-1.98]). IGG-Clin was predictive of recurrence (pooled HR = 2.11, [1.75-2.55], I2 = 0%) and death (pooled HR = 1.99, 95% [0.84-4.73], I2 = 79%) across cohorts. IGG was associated with adaptive immune response at CIBERSORTx and EcoTyper analysis.
Interpretation: IGG is linked to improved prognosis and pCR in early-stage TNBC. The integration of IGG alongside tumor and nodal staging holds promise as an approach to identify patients benefitting from intensified or de-intensified treatments.
Funding: This study received funding from: Associació Beca Marta Santamaria, European Union's Horizon 2020 research and innovation and Marie Skłodowska-Curie Actions programs, Fundación FERO, Fundación CRIS contra el cáncer, Agència de Gestó d'Ajuts Universitaris i de Recerca, Instituto de Salud Carlos III, Fundación Contigo, Asociación Cáncer de Mama Metastásico IV, Breast Cancer Research Foundation, RESCUER, Fundación científica AECC and FSEOM.
Keywords: B-cell/immunoglobulin signature (IGG); Event-free survival (EFS); Gene expression; Overall survival (OS); Pathological complete response (pCR); Predictive biomarkers; Prognostic biomarkers; Triple-negative breast cancer (TNBC).
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests B. Conte reports speaker fees from Veracyte and payment for educational events from Medsite and Novartis. A. Prat reports consulting fees from Roche, Pfizer, Novartis, Amgen, BMS, Puma, Oncolytics Biotech, MSD, Guardant Health, Peptomyc and Lilly, lecture fees from Roche, Pfizer, Novartis, Amgen, BMS, Nanostring Technologies and Daiichi Sankyo; patents filed PCT/EP2016/080056, PCT/EP2022/086493, PCT/EP2023/060810, EP23382703 and EP23383369; stockholder and consultant of Reveal Genomics, SL; and institutional financial interests from Boehringer, Novartis, Roche, Nanostring, Sysmex Europa GmbH, Medica Scientia Innovation Research, SL, Celgene, Astellas and Pfizer. F. Schettini has declared consulting fees from Pfizer, honoraria for lectures from Novartis, Gilead and Daiichy Sankyo, and travel expenses from Novartis and Daiichy Sankyo. O. Martínez-Sáez has declared institutional grants from Roche; personal consulting fees from Roche and Reveal Genomics; honoraria for presentations by Daiichi Sankyo, Pierre Fabre, and Reveal Genomics; and travel expenses by Gilead, Pierre Fabre, Novartis, and MSD. A. Vivancos has declared institutional grants from Bristol Meyers Squibb, Incyte, and Roche; personal consulting fees from Bayer, Bristol Meyers Squibb (BMS); Guardant, Incyte, and Roche; and personal stock options from Reveal Genomics. F. Brasó-Maristany has patents filed: PCT/EP2022/086493, PCT/EP2023/060810, EP23382703 and EP23383369. J. Parker as declared individual and institutional royalties from Veracyte–Prosigna, consulting fees from Bristol Meyers Squibb, Reveal Genomics, and GeneCentric, and holds a patent for breast cancer subtyping. Additionally, he has an equity interest in Reveal Genomics. M. Vidal has declared honoraria for presentations from Novartis, Roche, Pfizer, and Daichii, and travel expenses from Roche and Pfizer. Additionally, she has participated on a Data Safety Monitoring Board or Advisory Board for Novartis and Roche. C. Perou has declared consulting fees and personal stock options from Reveal Genomics. T. Pascual has declared consulting fees from Novartis; honoraria from Novartis, Astra-zeneca, Veracyte, and Argenetics. I. Garcia-Fructuoso has declared honoraria for presentations from Novartis, Daiichi Sankyo, Esteve, GSK; and travel expenses from Novartis, Gilead, Daiichi Sankyo, Lilly, and BMS. L. Paré has declared contract from Reveal Genomics, a HER2DX patent filed (PCT/EP2022/086493), and the TNBCDX patent filed (EP23382703.9). M. Marín-Aguilera has declared contract from Reveal Genomics. P. Villagrasa has declared contract and personal stock options from Reveal Genomics, the HER2DX patent filed (PCT/EP2022/086493), and the DNADX patent filed (EP22382387.3). G. Villacampa has received a speaker's fee from Merck Sharp & Dohme, Pfizer, GlaxoSmithKline and Pierre Fabrer, and received consultant fees from Reveal Genomics. C. Falato is currently employed in AstraZeneca. The remaining authors declare no competing interests.
Figures






References
-
- Dent R., Trudeau M., Pritchard K.I., et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13:4429–4434. - PubMed
-
- Hudis C.A., Gianni L. Triple-negative breast cancer: an unmet medical need. Oncol. 2011;16(Suppl 1):1–11. - PubMed
-
- Korde L.A., Somerfield M.R., Hershman D.L. For the neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer guideline expert panel. Use of immune checkpoint inhibitor pembrolizumab in the treatment of high-risk, early-stage triple-negative breast cancer: ASCO guideline rapid recommendation update. J Clin Orthod. 2022;40:1696–1698. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
