

Expanding Critical Care Delivery beyond the Intensive Care Unit: Determining the Design and Implementation Needs for a Tele-Critical Care Consultation Service
- PMID: 38447966
- PMCID: PMC10917611
- DOI: 10.1055/s-0044-1780508
Expanding Critical Care Delivery beyond the Intensive Care Unit: Determining the Design and Implementation Needs for a Tele-Critical Care Consultation Service
Abstract
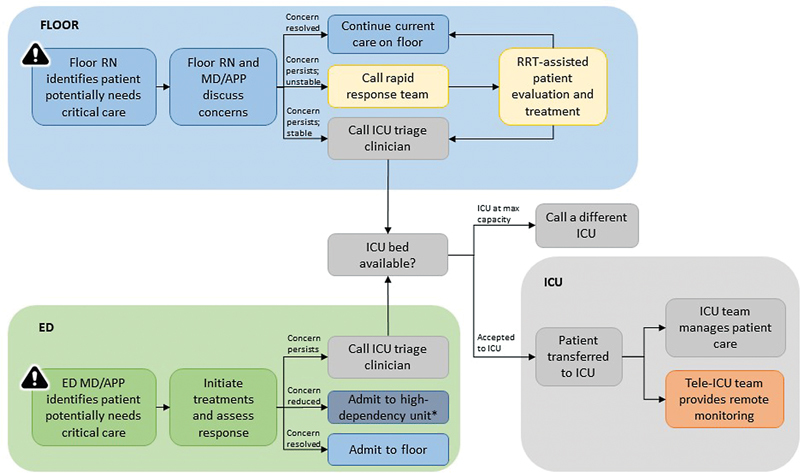
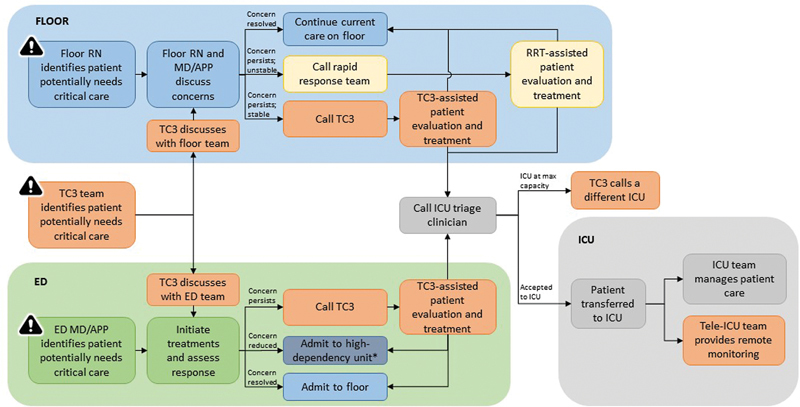
Background: Unplanned intensive care unit (ICU) admissions from medical/surgical floors and increased boarding times of ICU patients in the emergency department (ED) are common; approximately half of these are associated with adverse events. We explore the potential role of a tele-critical care consult service (TC3) in managing critically ill patients outside of the ICU and potentially preventing low-acuity unplanned admissions and also investigate its design and implementation needs.
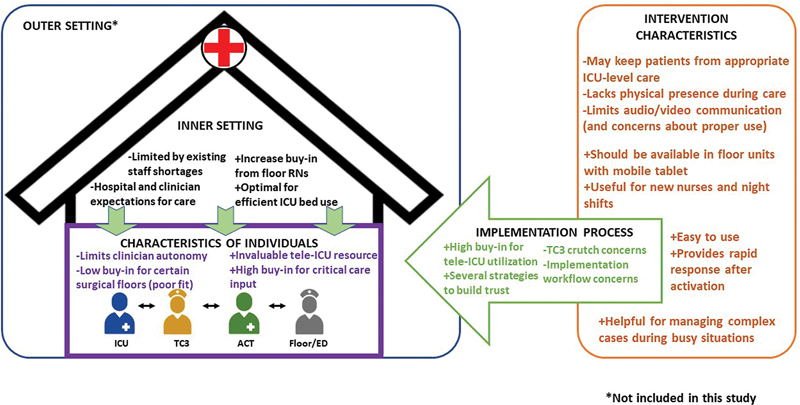
Methods: We conducted a qualitative study involving general observations of the units, shadowing of clinicians during patient transfers, and interviews with clinicians from the ED, medical/surgical floor units and their ICU counterparts, tele-ICU, and the rapid response team at a large academic medical center in St. Louis, Missouri, United States. We used a hybrid thematic analysis approach supported by open and structured coding using the Consolidated Framework for Implementation Research (CFIR).
Results: Over 165 hours of observations/shadowing and 26 clinician interviews were conducted. Our findings suggest that a tele-critical care consult (TC3) service can prevent avoidable, lower acuity ICU admissions by offering a second set of eyes via remote monitoring and providing guidance to bedside and rapid response teams in the care delivery of these patients on the floor/ED. CFIR-informed enablers impacting the successful implementation of the TC3 service included the optional and on-demand features of the TC3 service, around-the-clock availability, and continuous access to trained critical care clinicians for avoidable lower acuity (ALA) patients outside of the ICU, familiarity with tele-ICU staff, and a willingness to try alternative patient risk mitigation strategies for ALA patients (suggested by TC3), before transferring all unplanned admissions to ICUs. Conversely, the CFIR-informed barriers to implementation included a desire to uphold physician autonomy by floor/ED clinicians, potential role conflicts with rapid response teams, additional workload for floor/ED nurses, concerns about obstructing unavoidable, higher acuity admissions, and discomfort with audio-visual tools. To amplify these potential enablers and mitigate potential barriers to TC3 implementation, informed by this study, we propose two key characteristics-essential for extending the delivery of critical care services beyond the ICU-underlying a telemedicine critical care consultation model including its virtual footprint and on-demand and optional service features.
Conclusion: Tele-critical care represents an innovative strategy for delivering safe and high-quality critical care services to lower acuity borderline patients outside the ICU setting.
Thieme. All rights reserved.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Healthcare stakeholders' perceptions and experiences of factors affecting the implementation of critical care telemedicine (CCT): qualitative evidence synthesis.Cochrane Database Syst Rev. 2021 Feb 18;2(2):CD012876. doi: 10.1002/14651858.CD012876.pub2. Cochrane Database Syst Rev. 2021. PMID: 33599282 Free PMC article.
-
Implementation of Tele-Critical Care at General Leonard Wood Army Community Hospital.Mil Med. 2020 Feb 13;185(1-2):e191-e196. doi: 10.1093/milmed/usz147. Mil Med. 2020. PMID: 31247104
-
Staff acceptance of a telemedicine intensive care unit program: a qualitative study.J Crit Care. 2013 Dec;28(6):890-901. doi: 10.1016/j.jcrc.2013.05.008. Epub 2013 Jul 30. J Crit Care. 2013. PMID: 23906904
-
Telemedicine in the ICU: Innovation in the Critical Care Process.J Intensive Care Med. 2021 Dec;36(12):1377-1384. doi: 10.1177/0885066620968518. Epub 2020 Oct 28. J Intensive Care Med. 2021. PMID: 33111599
-
Integrating a Virtual ICU with Cardiac and Cardiovascular ICUs: Managing the Needs of a Complex and High-Acuity Specialty ICU Cohort.Methodist Debakey Cardiovasc J. 2023 Aug 1;19(4):4-16. doi: 10.14797/mdcvj.1247. eCollection 2023. Methodist Debakey Cardiovasc J. 2023. PMID: 37547898 Free PMC article. Review.
Cited by
-
An Explanatory Mixed-Methods Study of Intensive Care Unit Net Benefit: Triage and Trajectory for Sepsis and Acute Respiratory Failure.Ann Am Thorac Soc. 2025 Apr;22(4):570-580. doi: 10.1513/AnnalsATS.202408-806OC. Ann Am Thorac Soc. 2025. PMID: 39773160
-
Communication Challenges Experienced by Clinicians and Patients during Teleconsultation: A Scoping Review.Appl Clin Inform. 2025 Jan;16(1):56-66. doi: 10.1055/a-2425-8626. Epub 2024 Sep 30. Appl Clin Inform. 2025. PMID: 39348865
References
-
- Barrett M L, Smith M W, Elixhauser A, Honigman L S, Pines J M.Utilization of Intensive Care Services, 2011Rockville, MD:Agency for Healthcare Research and Quality (US); 2006 - PubMed
-
- Groeger J S, Guntupalli K K, Strosberg M et al.Descriptive analysis of critical care units in the United States: patient characteristics and intensive care unit utilization. Crit Care Med. 1993;21(02):279–291. - PubMed
-
- Mulvey H E, Haslam R D, Laytin A D, Diamond C A, Sims C A. Unplanned ICU admission is associated with worse clinical outcomes in geriatric trauma patients. J Surg Res. 2020;245:13–21. - PubMed
-
- Rubano J A, Vosswinkel J A, McCormack J E, Huang E C, Shapiro M J, Jawa R S. Unplanned intensive care unit admission following trauma. J Crit Care. 2016;33:174–179. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
