

Utility of Diffusion-weighted MR Imaging for Evaluating the Depth of Invasion in Oral Tongue Squamous Cell Carcinoma
- PMID: 38447989
- PMCID: PMC11996252
- DOI: 10.2463/mrms.mp.2023-0137
Utility of Diffusion-weighted MR Imaging for Evaluating the Depth of Invasion in Oral Tongue Squamous Cell Carcinoma
Abstract
Purpose: The 8th edition of the American Joint Committee on Cancer staging system included the depth of invasion (DOI) for the T classification of oral cancer. However, no standardized method has been established to clinically measure the DOI. This study aimed to investigate the accuracy of MRI-based DOI for oral tongue squamous cell carcinoma (OTSCC) in each MRI sequence.
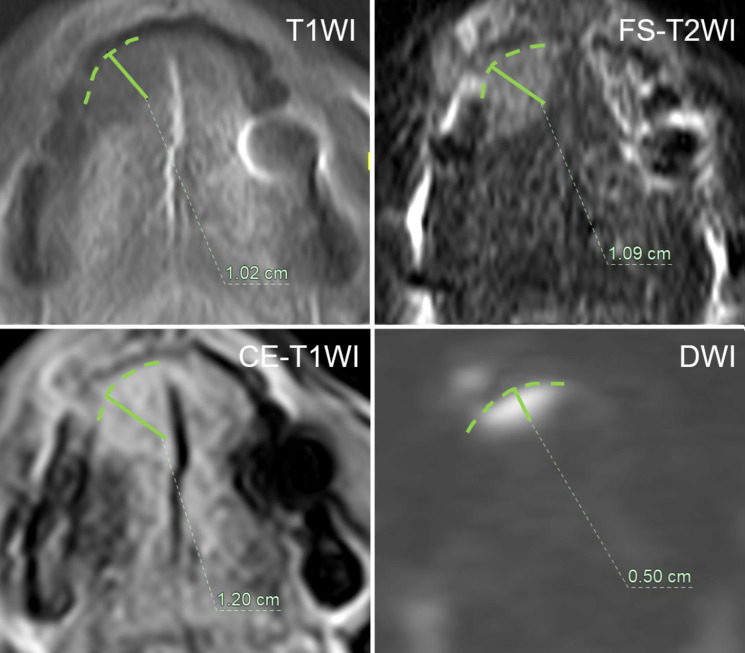
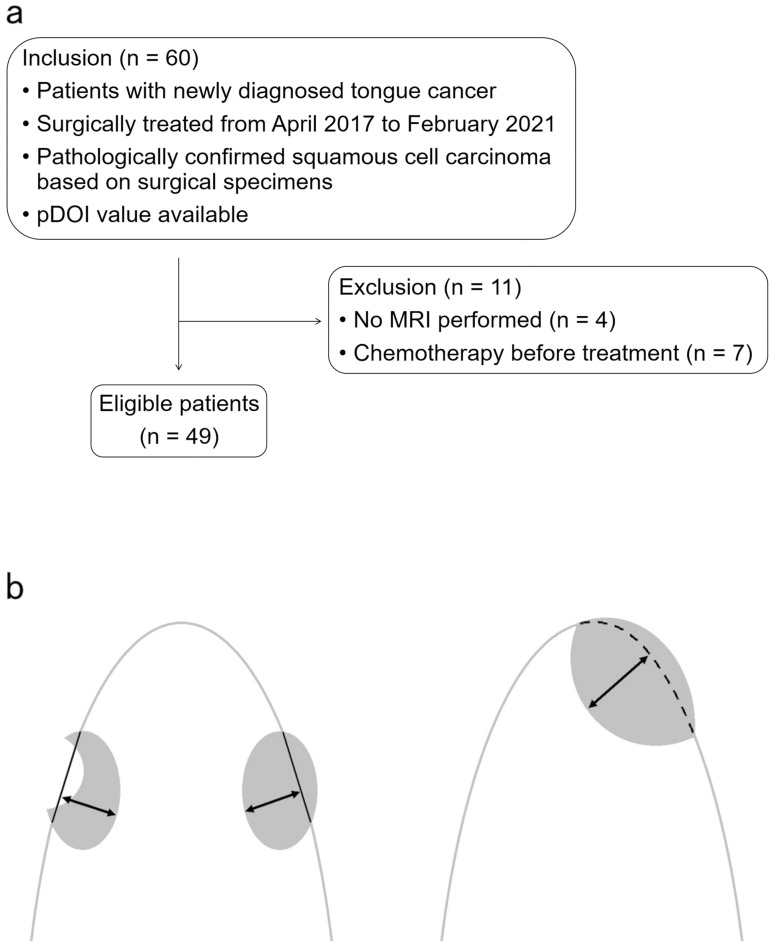
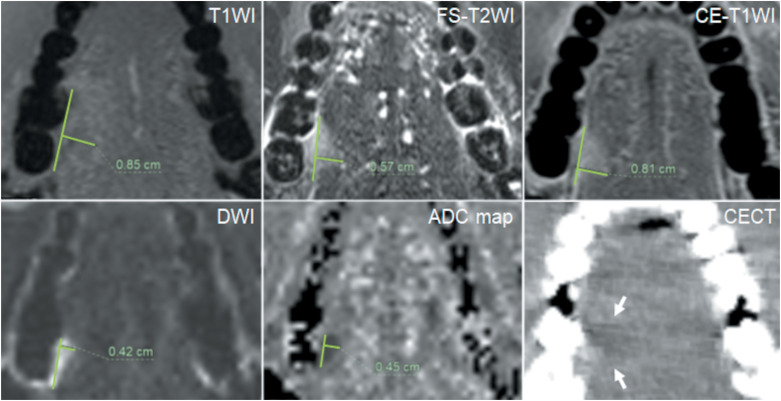
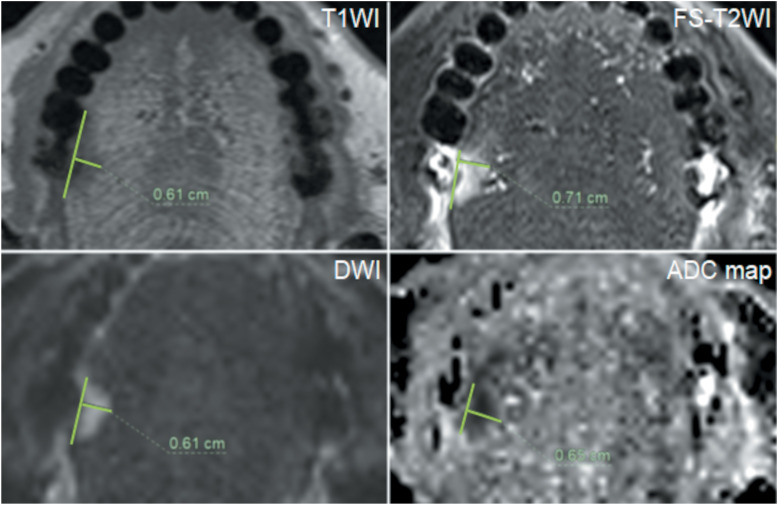
Methods: We enrolled 49 patients with histologically proven OTSCC, treated surgically between April 2017 and February 2021. We divided the DOI into three groups using 5 and 10 mm, the thresholds for determining the T stage, and retrospectively evaluated the agreement between MRI-based DOI and pathological DOI (pDOI) for each MRI sequence, axial T1-weighted imaging (T1WI), T2-weighted imaging with fat suppression (FS-T2WI), contrast-enhanced T1WI with fat suppression (CE-T1WI), diffusion-weighted imaging (DWI), and apparent diffusion coefficient (ADC) maps. We also divided the DOI into two groups using 3 mm, the threshold for considering elective neck dissection, and evaluated the overestimation rate of MRI-based DOI in lesions with pDOI ≤ 3 mm.
Results: With 5-mm and 10-mm divisions, the accuracy of the DOI assessment was highest on DWI (0.82, weighted kappa = 0.85). With a 3-mm division, the accuracy was also highest on DWI (0.87, kappa = 0.73). The overestimation rate of the MRI-based DOI in lesions with pDOI ≤ 3 mm was lowest on DWI (27.8%).
Conclusion: DOI on DWI exhibits a comparatively higher rate of concordance with pDOI. DWI may be more useful than other MRI sequences in evaluating the DOI of OTSCC.
Keywords: depth of invasion; diffusion-weighted imaging; magnetic resonance imaging; oral cancer; squamous cell carcinoma.
Figures

References
-
- Machiels JP, René Leemans C, Golusinski W, Grau C, Licitra L, Gregoire V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2020; 31:1462–1475. - PubMed
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71:209–249. - PubMed
-
- Japan Society for Head and Neck Cancer, Cancer Registry Committee. Report of head and neck cancer registry of japan clinical statistics of registered patients, 2019. http://www.jshnc.umin.ne.jp/pdf/HNCreport_2019.pdf
-
- Ridge JA, Lydiatta WM, Patel SG, et al. Lip and oral cavity. In: Amin MB. Edge S, Greene F, Byrd DR, Brookland RK, Washington MKet al. , editors. AJCC cancer staging manual. 8th ed. New York: Springer, 2017; 79-94.