

Protocol for venoarterial ExtraCorporeal Membrane Oxygenation to reduce morbidity and mortality following bilateral lung TransPlantation: the ECMOToP randomised controlled trial
- PMID: 38448059
- PMCID: PMC10916175
- DOI: 10.1136/bmjopen-2023-077770
Protocol for venoarterial ExtraCorporeal Membrane Oxygenation to reduce morbidity and mortality following bilateral lung TransPlantation: the ECMOToP randomised controlled trial
Abstract
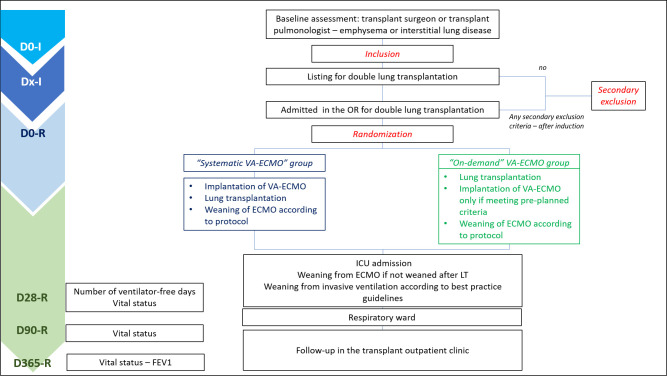
Introduction: Lung transplantation (LTx) aims at improving survival and quality of life for patients with end-stage lung diseases. Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is used as intraoperative support for LTx, despite no precise guidelines for its initiation. We aim to evaluate two strategies of VA-ECMO initiation in the perioperative period in patients with obstructive or restrictive lung disease requiring bilateral LTx. In the control 'on-demand' arm, high haemodynamic and respiratory needs will dictate VA-ECMO initiation; in the experimental 'systematic' arm, VA-ECMO will be pre-emptively initiated. We hypothesise a 'systematic' strategy will increase the number of ventilatory-free days at day 28.
Methods and analysis: We designed a multicentre randomised controlled trial in parallel groups. Adult patients with obstructive or restrictive lung disease requiring bilateral LTx, without a formal indication for pre-emptive VA-ECMO before LTx, will be included. Patients with preoperative pulmonary hypertension with haemodynamic collapse, ECMO as a bridge to transplantation, severe hypoxaemia or hypercarbia will be secondarily excluded. In the systematic group, VA-ECMO will be systematically implanted before the first pulmonary artery cross-clamp. In the on-demand group, VA-ECMO will be implanted intraoperatively if haemodynamic or respiratory indices meet preplanned criteria. Non-inclusion, secondary exclusion and VA-ECMO initiation criteria were validated by a Delphi process among investigators. Postoperative weaning of ECMO and mechanical ventilation will be managed according to best practice guidelines. The number of ventilator-free days at 28 days (primary endpoint) will be compared between the two groups in the intention-to-treat population. Secondary endpoints encompass organ failure occurrence, day 28, day 90 and year 1 vital status, and adverse events.
Ethics and dissemination: The sponsor is the Assistance Publique-Hôpitaux de Paris. The ECMOToP protocol version 2.1 was approved by Comité de Protection des Personnes Ile de France VIII. Results will be published in international peer-reviewed medical journals.
Trial registration number: NCT05664204.
Keywords: Adult anaesthesia; Randomized Controlled Trial; Thoracic surgery; Transplant surgery.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JM declares congress reimbursement fees from Biotest. PMor declares consulting fees from iPerf. PMon declares lecture honoraria and board fees from Pfizer, MSD and Menarini. PE, DB, AC, JF, JJ, PL, OM, PP, HR, ES, JT, FT, MV, YC and HM declare no competing interest.
Figures
References
-
- Snell GI, Yusen RD, Weill D, et al. . Report of the ISHLT working group on primary lung graft dysfunction, part I: definition and grading-A 2016 consensus group statement of the International society for heart and lung transplantation. J Heart Lung Transplant 2017;36:1097–103. 10.1016/j.healun.2017.07.021 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical