

Differences of respiratory mechanics in mechanical ventilation of acute respiratory distress syndrome between patients with COVID-19 and Influenza A
- PMID: 38448933
- PMCID: PMC10919012
- DOI: 10.1186/s12931-024-02730-4
Differences of respiratory mechanics in mechanical ventilation of acute respiratory distress syndrome between patients with COVID-19 and Influenza A
Abstract
Background: Whether COVID-19-induced acute respiratory distress syndrome (ARDS) should be approached differently in terms of mechanical ventilation therapy compared to other virus-induced ARDS is debatable. Therefore, we aimed to ascertain whether the respiratory mechanical characteristics of COVID-19-induced ARDS differ from those of influenza A induced ARDS, in order to establish a rationale for mechanical ventilation therapy in COVID-19-induced ARDS.
Methods: This was a retrospective cohort study comparing patients with COVID-19-induced ARDS and influenza A induced ARDS. We included intensive care unit (ICU) patients with COVID-19 or Influenza A aged ≥ 19, who were diagnosed with ARDS according to the Berlin definition between January 2015 and July 2021. Ventilation parameters for respiratory mechanics were collected at specific times on days one, three, and seven after intubation.
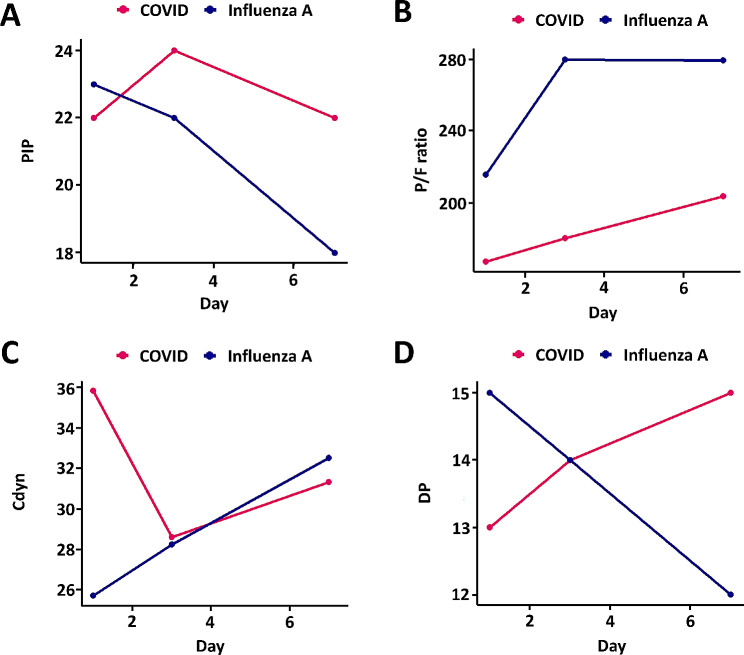
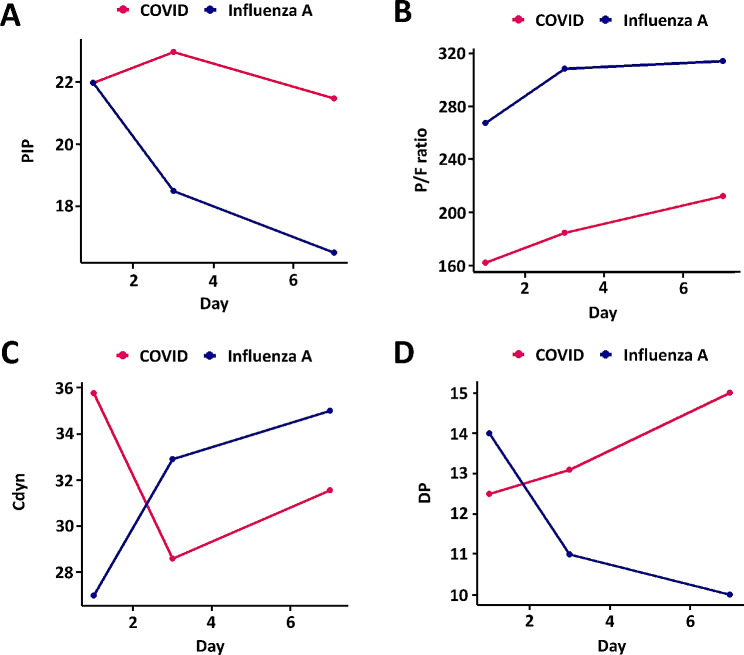
Results: The median age of the 87 participants was 71.0 (62.0-78.0) years old, and 63.2% were male. The ratio of partial pressure of oxygen in arterial blood to the fractional of inspiratory oxygen concentration in COVID-19-induced ARDS was lower than that in influenza A induced ARDS during the initial stages of mechanical ventilation (influenza A induced ARDS 216.1 vs. COVID-19-induced ARDS 167.9, p = 0.009, day 1). The positive end expiratory pressure remained consistently higher in the COVID-19 group throughout the follow-up period (7.0 vs. 10.0, p < 0.001, day 1). COVID-19 and influenza A initially showed different directions for peak inspiratory pressure and dynamic compliance; however, after day 3, both groups exhibited similar directions. Dynamic driving pressure exhibited opposite trends between the two groups during mechanical ventilation.
Conclusions: Respiratory mechanics show clear differences between COVID-19-induced ARDS and influenza A induced ARDS. Based on these findings, we can consider future treatment strategies for COVID-19-induced ARDS.
Keywords: Acute respiratory distress syndrome; COVID-19; Influenza A; Mechanical ventilation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Longitudinal changes in compliance, oxygenation and ventilatory ratio in COVID-19 versus non-COVID-19 pulmonary acute respiratory distress syndrome.Crit Care. 2021 Jul 15;25(1):248. doi: 10.1186/s13054-021-03665-8. Crit Care. 2021. PMID: 34266454 Free PMC article.
-
[Analysis of clinical treatment of acute respiratory distress syndrome assisted by artificial intelligence].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Apr;36(4):369-376. doi: 10.3760/cma.j.cn121430-20231027-00916. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38813630 Chinese.
-
Comparing Clinical Outcomes of COVID-19 and Influenza-Induced Acute Respiratory Distress Syndrome: A Propensity-Matched Analysis.Viruses. 2023 Apr 5;15(4):922. doi: 10.3390/v15040922. Viruses. 2023. PMID: 37112902 Free PMC article.
-
Effect of prone positioning on oxygenation and static respiratory system compliance in COVID-19 ARDS vs. non-COVID ARDS.Respir Res. 2021 Aug 6;22(1):220. doi: 10.1186/s12931-021-01819-4. Respir Res. 2021. PMID: 34362368 Free PMC article. Review.
-
Mechanical ventilation parameters in critically ill COVID-19 patients: a scoping review.Crit Care. 2021 Mar 20;25(1):115. doi: 10.1186/s13054-021-03536-2. Crit Care. 2021. PMID: 33743812 Free PMC article.
Cited by
-
Comparative Evaluation of Risk of Death in Mechanically Ventilated Patients With COVID-19 and Influenza: A Population-Based Cohort Study.J Clin Med Res. 2025 Apr;17(4):187-199. doi: 10.14740/jocmr6189. Epub 2025 Mar 17. J Clin Med Res. 2025. PMID: 40322716 Free PMC article.
References
-
- Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307:2526–33. - PubMed
-
- Hasan SS, Capstick T, Ahmed R, Kow CS, Mazhar F, Merchant HA, Zaidi STR. Mortality in COVID-19 patients with acute respiratory distress syndrome and corticosteroids use: a systematic review and meta-analysis. Expert Rev Respir Med. 2020;14:1149–63. doi: 10.1080/17476348.2020.1804365. - DOI - PMC - PubMed
-
- Hariri LP, North CM, Shih AR, Israel RA, Maley JH, Villalba JA, Vinarsky V, Rubin J, Okin DA, Sclafani A, et al. Lung histopathology in Coronavirus Disease 2019 as compared with severe Acute Respiratory Sydrome and H1N1 Influenza: a systematic review. Chest. 2021;159:73–84. doi: 10.1016/j.chest.2020.09.259. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
