

Progress in controlling the transmission of schistosome parasites in Southern Ethiopia: the Geshiyaro Project in the Wolaita Zone
- PMID: 38448997
- PMCID: PMC10919034
- DOI: 10.1186/s13071-024-06156-1
Progress in controlling the transmission of schistosome parasites in Southern Ethiopia: the Geshiyaro Project in the Wolaita Zone
Erratum in
-
Correction: Progress in controlling the transmission of schistosome parasites in Southern Ethiopia: the Geshiyaro Project in the Wolaita Zone.Parasit Vectors. 2024 Mar 28;17(1):158. doi: 10.1186/s13071-024-06251-3. Parasit Vectors. 2024. PMID: 38549079 Free PMC article. No abstract available.
Abstract
Background: This paper describes changes in the prevalence and intensity of schistosome parasite infections in a project integrating mass drug administration (MDA), water, sanitation, and hygiene (WaSH), and behavioral change interventions.
Methods: The Geshiyaro Project comprises three intervention arms. Arm 1 is subdivided into "Arm 1 pilot" (one district) and Arm 1 (four other districts), both receiving integrated community-wide MDA with intensive WaSH interventions. Arm 2 involves 17 districts with community-wide MDA interventions, while Arm 3 serves as a control with school-based MDA interventions in three districts. A total of 150 individuals, stratified by age group, were randomly selected from each of the 45 sentinel sites. Arm sizes were 584 (Arm 1 pilot), 1636 (Arm 1), 2203 (Arm 2), and 2238 (Arm 3). Statistical tests were employed to compare infection prevalence and intensity across the different arms.
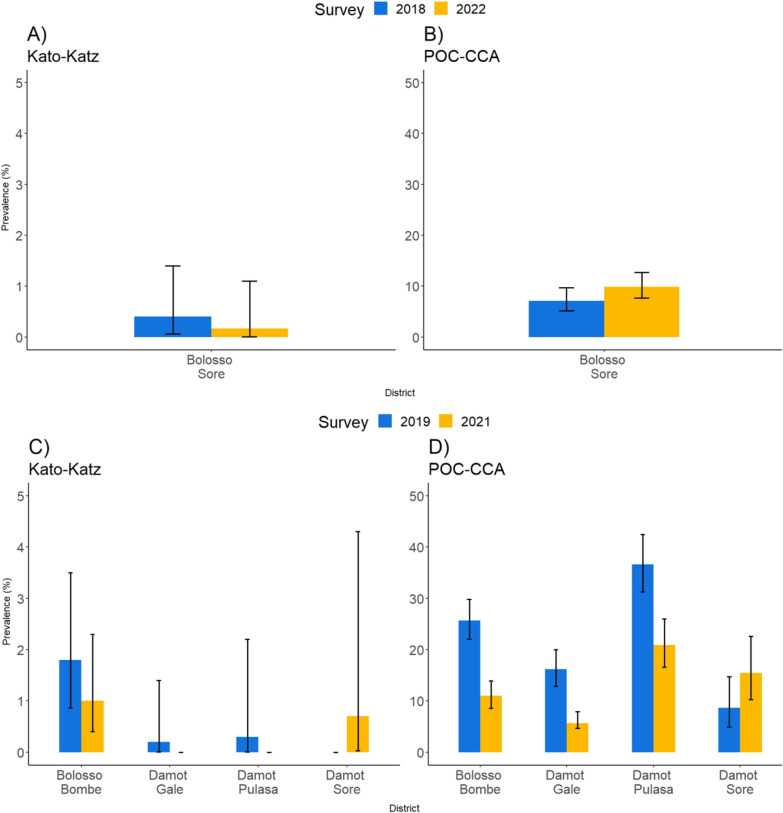
Results: The prevalence of schistosome parasite infection ranged from 0% to 2.6% and from 1.7% to 25.7% across districts, employing the Kato-Katz (KK) and point-of-care circulating cathodic antigen (POC-CCA) diagnostics, respectively. The mean infection intensity level showed no marked difference between baseline and follow-up surveys when measured by KK, except in Arm 2 (t = 6.89, P < 0.0001). Infection prevalence decreased significantly in Arm 1 (t = 8.62, P < 0.0001), Arm 2 (t = 6.94, P < 0.0001), and Arm 3 (t = 8.83, P < 0.0001), but not in Arm 1 pilot (t = 1.69, P = 0.09) by POC-CCA, when trace was considered positive. The decrease was significant only in Arm 1 (t = 3.28, P = 0.0001) and Arm 2 (t = 7.62, P < 0.0001) when the trace was considered negative in POC-CCA. Arm 2 demonstrated a significant difference in difference (DID) compared to the control group, Arm 3, regardless of whether trace in POC-CCA was considered positive (DID = 3.9%, df = 8780, P = 0.025) or negative (DID = -5.2, df = 8780, P = 0.0004).
Conclusions: The prevalence of schistosomiasis was low when employing the KK diagnostic but moderate in some locations by the POC-CCA diagnostic. The infection level had decreased across all arms of the Geshiyaro study at mid-term of the 7-year project, but further efforts are needed to reduce the rate of parasite transmission based on the POC-CCA diagnostic scores.
Keywords: Kato-Katz (KK); Mass drug administration (MDA); Point-of-care circulating cathodic antigen (POC-CCA); Schistosomiasis (SCH).
© 2024. Crown.
Conflict of interest statement
None declared.
Figures



References
-
- WHO. Ending the neglect to attain the Sustainable Development Goals: a road map for neglected tropical diseases 2021–2030. Word Heal Organ. 2020. https://www.who.int/publications/i/item/9789240010352. Accessed 2 Aug 2022.
-
- Hotez PJ, Bundy DAP, Beegle K, Brooker S, Drake L, Silva N de, et al. Chapter 24. Helminth infections: soil-transmitted helminth infections and schistosomiasis. Disease Control Priorities in Developing Countries (2nd edition). The International Bank for Reconstruction and Development/The World Bank; 2006. 467–82. https://www.ncbi.nlm.nih.gov/books/NBK11748/. Accessed 28 Aug 2022.
-
- WHO. Who guideline on control and elimination of human schistosomiasis. 2022. - PubMed
-
- Press Release European medicines agency validates application for arpraziquantel to treat schistosomiasis in preschool-aged children. www.pediatricpraziquantelconsortium.org. Accessed 22 Mar 22.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
