

Simpson's Grading Scale for WHO Grade I Meningioma Resection in the Modern Neurosurgical Era: Are We Really Asking the Right Question?
- PMID: 38449587
- PMCID: PMC10914467
- DOI: 10.1055/a-2021-8852
Simpson's Grading Scale for WHO Grade I Meningioma Resection in the Modern Neurosurgical Era: Are We Really Asking the Right Question?
Abstract
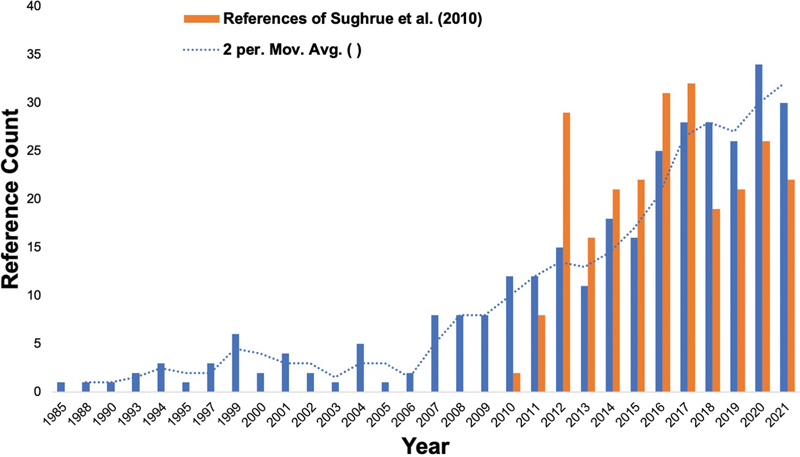
The Simpson grading scale for the classification of the extent of meningioma resection provided a tremendous movement forward in 1957 suggesting increasing the extent of resection improves recurrence rates. However, equal, if not greater, movements forward have been made in the neurosurgical community over the last half a century owing to improvements in neuroimaging capabilities, microsurgical techniques, and radiotherapeutic strategies. Sughrue et al proposed the idea that these advancements have altered what a "recurrence" and "subtotal resection" truly means in modern neurosurgery compared with Simpson's era, and that a mandated use of the Simpson Scale is likely less clinically relevant today. A subsequent period of debate ensued in the literature which sought to re-examine the clinical value of using the Simpson Scale in modern neurosurgery. While a large body of evidence has recently been provided, these data generally continue to support the clinical importance of gross tumor resection as well as the value of adjuvant radiation therapy and the importance of recently updated World Health Organization classifications. However, there remains a negligible interval benefit in performing overly aggressive surgery and heroic maneuvers to remove the last bit of tumor, dura, and/or bone just for the simple act of achieving a lower Simpson score. Ultimately, meningioma surgery may be better contextualized as a continuous set of weighted risk-benefit decisions throughout the entire operation.
Keywords: Simpson Scale; gross total resection; meningiomas; neuroimaging; neurosurgery; recurrence; subtotal resection.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest Michael Sughrue is the Chief Medical Officer and co-founder of Omniscient Neurotechnology and stakeholder. No products related to this were discussed in this paper. Nicholas Dadario has no conflicts of interest.
Figures
Similar articles
-
The relevance of Simpson Grade I and II resection in modern neurosurgical treatment of World Health Organization Grade I meningiomas.J Neurosurg. 2010 Nov;113(5):1029-35. doi: 10.3171/2010.3.JNS091971. Epub 2010 Apr 9. J Neurosurg. 2010. PMID: 20380529
-
The Simpson Grading: Is It Still Valid?Cancers (Basel). 2022 Apr 15;14(8):2007. doi: 10.3390/cancers14082007. Cancers (Basel). 2022. PMID: 35454912 Free PMC article. Review.
-
The role of Simpson grading in meningiomas after integration of the updated WHO classification and adjuvant radiotherapy.Neurosurg Rev. 2021 Aug;44(4):2329-2336. doi: 10.1007/s10143-020-01428-7. Epub 2020 Oct 26. Neurosurg Rev. 2021. PMID: 33104905 Free PMC article.
-
Relevance of Simpson grading system and recurrence-free survival after surgery for World Health Organization Grade I meningioma.J Neurosurg. 2017 Jan;126(1):201-211. doi: 10.3171/2016.1.JNS151842. Epub 2016 Apr 8. J Neurosurg. 2017. PMID: 27058201
-
Grading meningioma resections: the Simpson classification and beyond.Acta Neurochir (Wien). 2024 Jan 23;166(1):28. doi: 10.1007/s00701-024-05910-9. Acta Neurochir (Wien). 2024. PMID: 38261164 Free PMC article. Review.
References
-
- Sughrue M E, Kane A J, Shangari G et al.The relevance of Simpson Grade I and II resection in modern neurosurgical treatment of World Health Organization Grade I meningiomas. J Neurosurg. 2010;113(05):1029–1035. - PubMed
-
- Oya S, Kawai K, Nakatomi H, Saito N. Significance of Simpson grading system in modern meningioma surgery: integration of the grade with MIB-1 labeling index as a key to predict the recurrence of WHO Grade I meningiomas. J Neurosurg. 2012;117(01):121–128. - PubMed
-
- Hasseleid B F, Meling T R, Rønning P, Scheie D, Helseth E. Surgery for convexity meningioma: Simpson Grade I resection as the goal: clinical article. J Neurosurg. 2012;117(06):999–1006. - PubMed
