

Hepatocellular carcinoma in a transplanted donor liver and colon cancer developing in a patient with a complex background: A case report
- PMID: 38449797
- PMCID: PMC10915803
- DOI: 10.3892/ol.2024.14301
Hepatocellular carcinoma in a transplanted donor liver and colon cancer developing in a patient with a complex background: A case report
Abstract
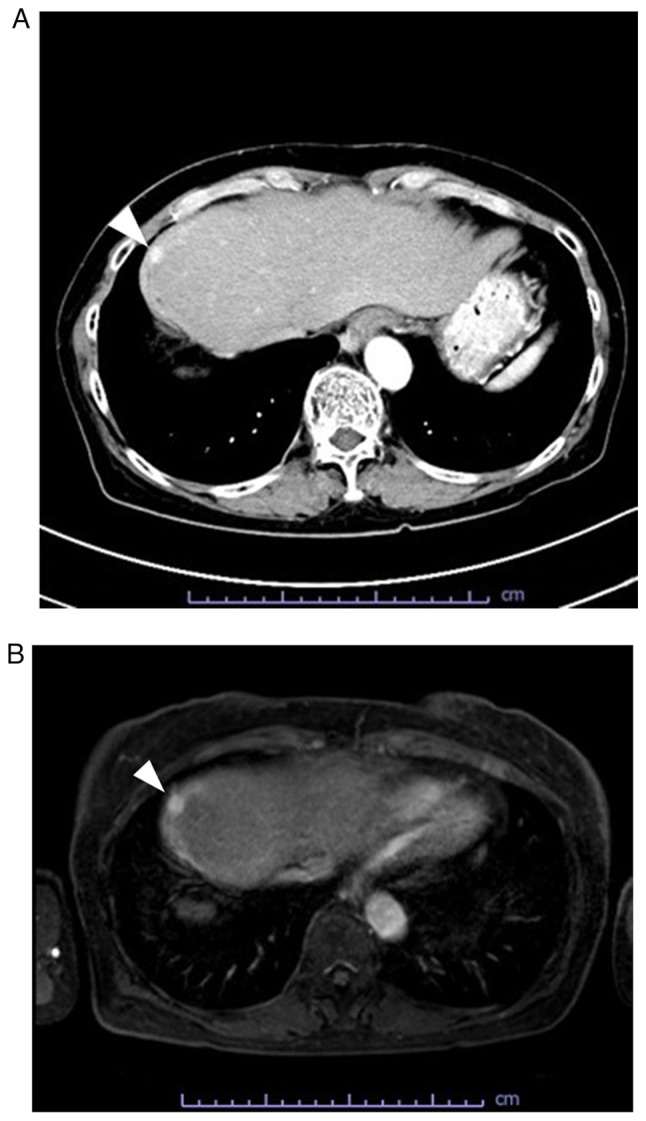
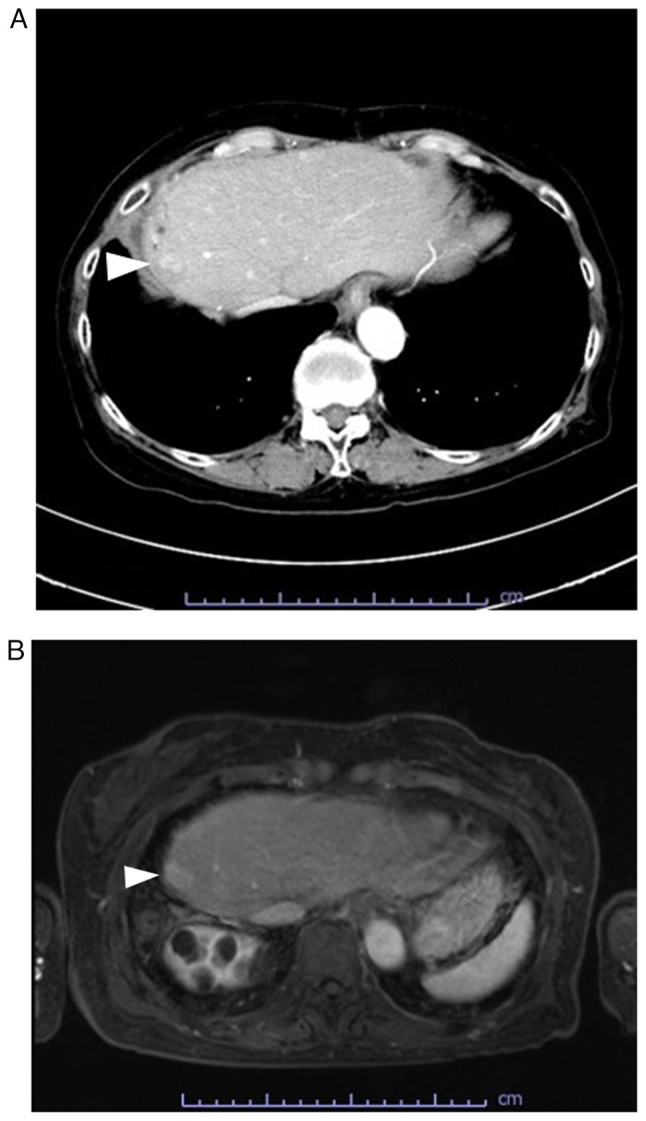
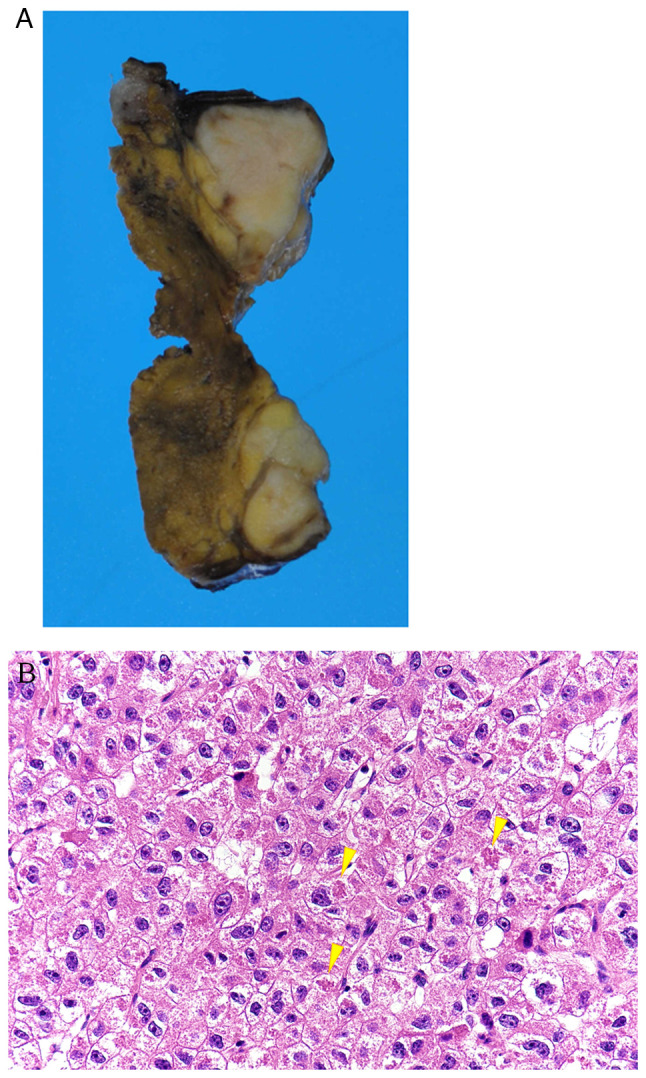
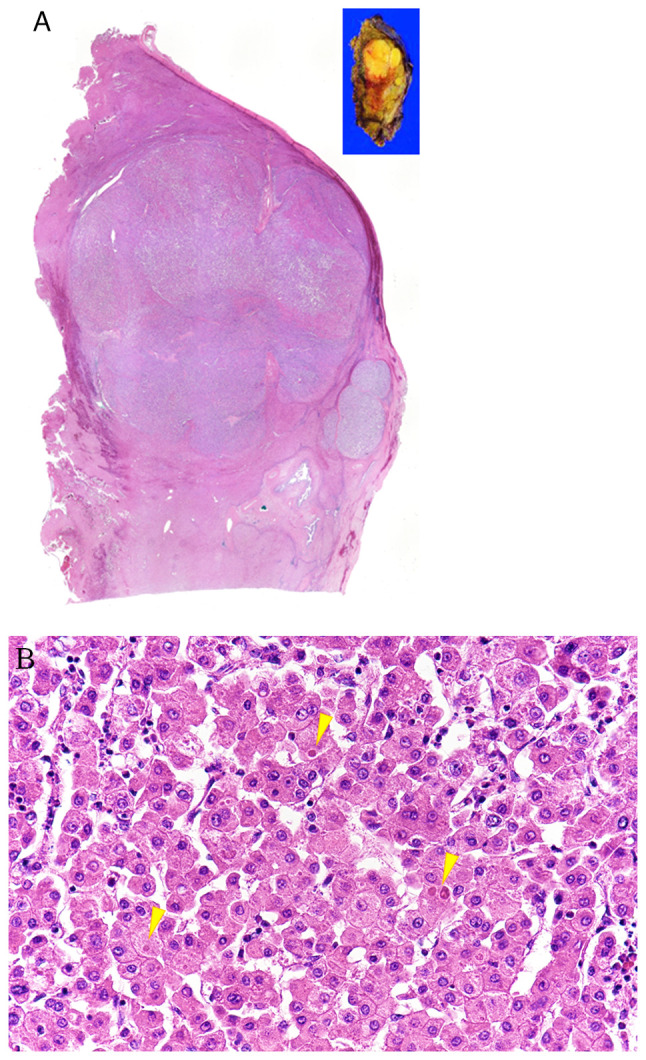
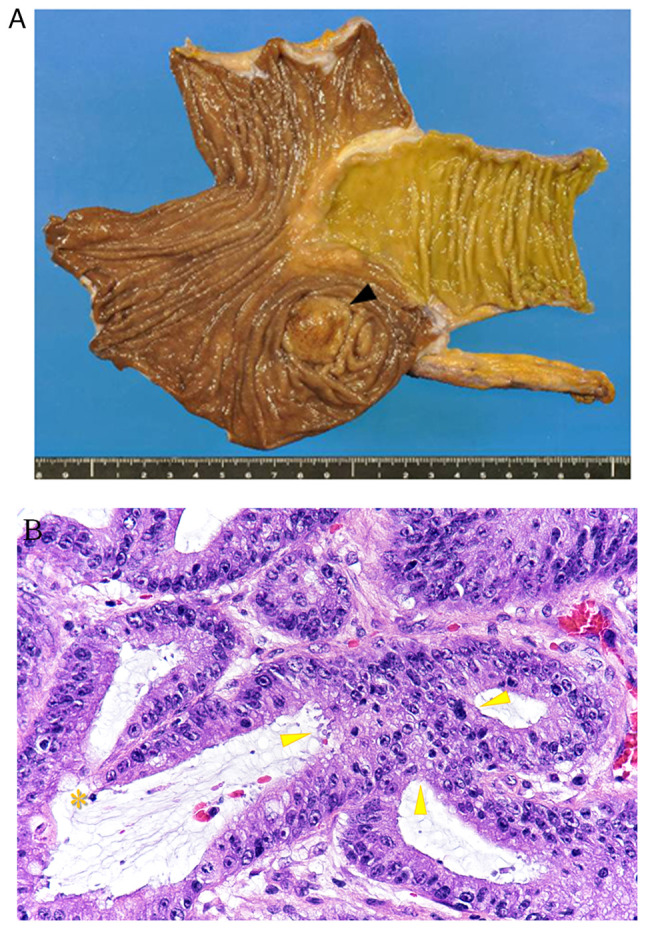
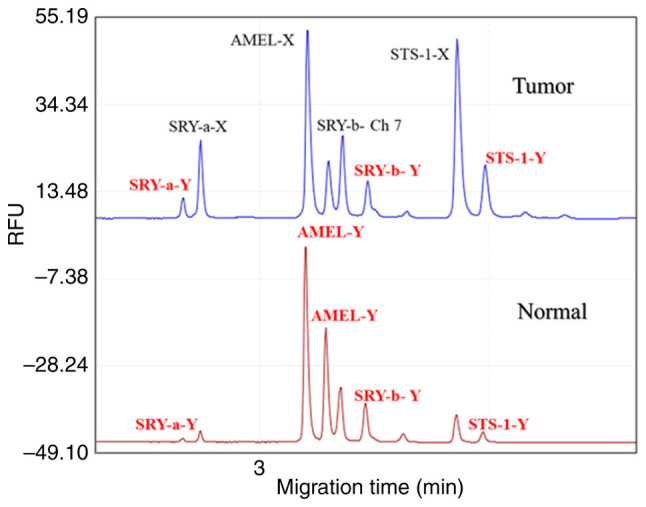
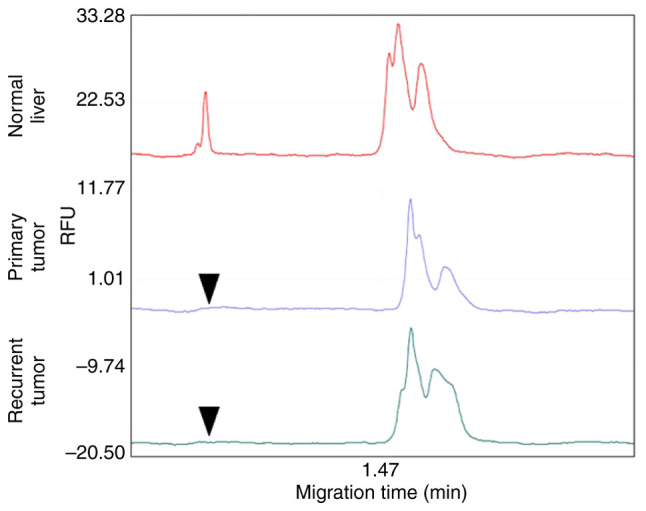
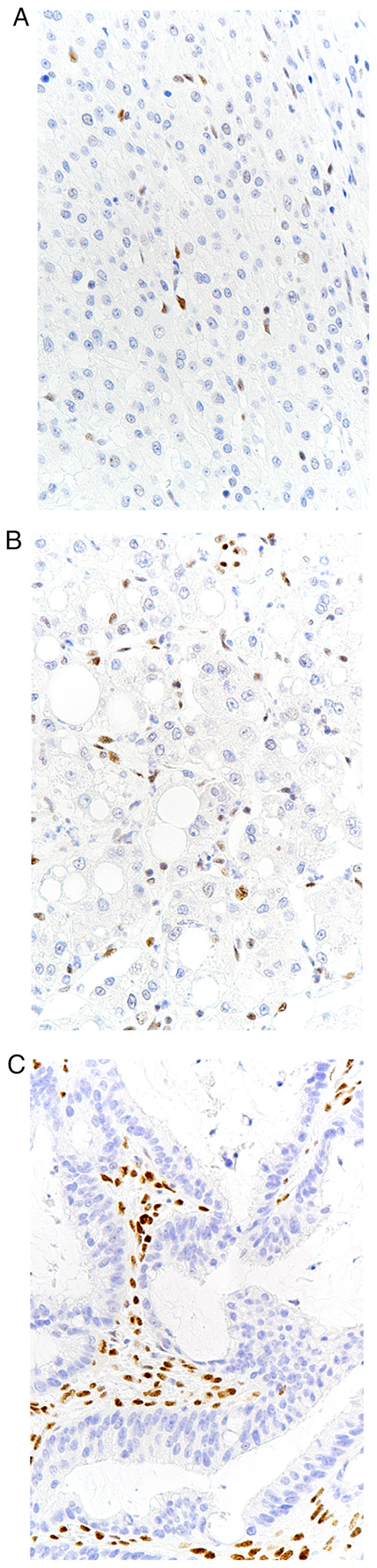
The development of tumors in livers transplanted from hepatitis B virus (HBV)-negative donors to patients with hepatitis B and cirrhosis is rare. The present study describes the case of a woman in her 60s who developed hepatocellular carcinoma (HCC) in her grafted liver, 19 years after transplantation, as well as a metachronous colorectal tumor. The pathological findings, including clinical, immunohistochemical and molecular results, are described in the present case report. The liver tumor was a conventional HCC and the colorectal tumor comprised a tubular adenocarcinoma. Immunohistochemistry of both tumors showed a loss of expression of mutL homolog 1 and postmeiotic segregation increased 2 in the tumor cells, confirming microsatellite instability-high (MSI-H) status. Furthermore, a molecular study detected the presence of genes located on the Y chromosome in the normal and tumor tissues of the liver, proving that the HCC occurred in the grafted liver. The present report also discusses that prolonged use of immunosuppressive drugs to prevent post-transplant rejection, poorly controlled diabetes mellitus and MSI-H may have contributed to the risk of tumor development.
Keywords: HBV; HCC; MSI; colon cancer; diabetes mellitus; immunosuppressant; transplantation.
Copyright: © 2024 Sumiyoshi et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Microsatellite instability mutator phenotype in hepatocellular carcinoma in non-alcoholic and non-virally infected normal livers.Carcinogenesis. 2004 Apr;25(4):541-7. doi: 10.1093/carcin/bgh035. Epub 2003 Dec 4. Carcinogenesis. 2004. PMID: 14656944
-
Long-term recurrence-free survival after liver transplantation from an ABO-incompatible living donor for treatment of hepatocellular carcinoma exceeding Milano criteria in a patient with hepatitis B virus cirrhosis: a case report.Transplant Proc. 2012 Mar;44(2):565-9. doi: 10.1016/j.transproceed.2012.01.029. Transplant Proc. 2012. PMID: 22410070
-
Hepatocellular carcinoma is associated with an increased risk of hepatitis B virus recurrence after liver transplantation.Gastroenterology. 2008 Jun;134(7):1890-9; quiz 2155. doi: 10.1053/j.gastro.2008.02.064. Epub 2008 Mar 4. Gastroenterology. 2008. PMID: 18424269 Clinical Trial.
-
State of the art treatment of hepatitis B virus hepatocellular carcinoma and the role of hepatitis B surface antigen post-liver transplantation and resection.Liver Int. 2022 Feb;42(2):288-298. doi: 10.1111/liv.15124. Epub 2021 Dec 20. Liver Int. 2022. PMID: 34846790 Free PMC article. Review.
-
Molecular mechanism of hepatocarcinogenesis.J Gastroenterol Hepatol. 1997 Oct;12(9-10):S309-13. doi: 10.1111/j.1440-1746.1997.tb00514.x. J Gastroenterol Hepatol. 1997. PMID: 9407351 Review.
References
Publication types
LinkOut - more resources
Full Text Sources