

Risk factors, prognostic factors, and nomograms for distant metastases in patients with gastroenteropancreatic neuroendocrine tumors: a population-based study
- PMID: 38449852
- PMCID: PMC10916283
- DOI: 10.3389/fendo.2024.1264952
Risk factors, prognostic factors, and nomograms for distant metastases in patients with gastroenteropancreatic neuroendocrine tumors: a population-based study
Abstract
Background: Patients with gastroenteropancreatic neuroendocrine tumors (GEP-NETs) have a poor prognosis for distant metastasis. Currently, there are no studies on predictive models for the risk of distant metastasis in GEP-NETs.
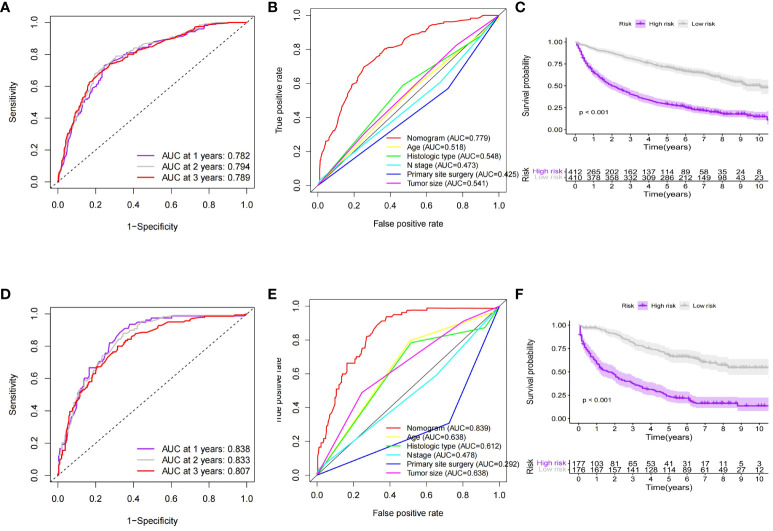
Methods: In this study, risk factors associated with metastasis in patients with GEP-NETs in the Surveillance, Epidemiology, and End Results (SEER) database were analyzed by univariate and multivariate logistic regression, and a nomogram model for metastasis risk prediction was constructed. Prognostic factors associated with distant metastasis in patients with GEP-NETs were analyzed by univariate and multivariate Cox, and a nomogram model for prognostic prediction was constructed. Finally, the performance of the nomogram model predictions is validated by internal validation set and external validation set.
Results: A total of 9145 patients with GEP-NETs were enrolled in this study. Univariate and multivariate logistic analysis demonstrated that T stage, N stage, tumor size, primary site, and histologic types independent risk factors associated with distant metastasis in GEP-NETs patients (p value < 0.05). Univariate and multivariate Cox analyses demonstrated that age, histologic type, tumor size, N stage, and primary site surgery were independent factors associated with the prognosis of patients with GEP-NETs (p value < 0.05). The nomogram model constructed based on metastasis risk factors and prognostic factors can predict the occurrence of metastasis and patient prognosis of GEP-NETs very effectively in the internal training and validation sets as well as in the external validation set.
Conclusion: In conclusion, we constructed a new distant metastasis risk nomogram model and a new prognostic nomogram model for GEP-NETs patients, which provides a decision-making reference for individualized treatment of clinical patients.
Keywords: SEER; distant metastasis; gastroenteropancreatic neuroendocrine tumors; nomogram; prognosis.
Copyright © 2024 Li, Fan, Tong and Lou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






Similar articles
-
Development and validation of predictive models for distant metastasis and prognosis of gastroenteropancreatic neuroendocrine neoplasms.Sci Rep. 2025 Mar 19;15(1):9510. doi: 10.1038/s41598-025-92974-x. Sci Rep. 2025. PMID: 40108260 Free PMC article.
-
Epidemiologic Trends of and Factors Associated With Overall Survival for Patients With Gastroenteropancreatic Neuroendocrine Tumors in the United States.JAMA Netw Open. 2021 Sep 1;4(9):e2124750. doi: 10.1001/jamanetworkopen.2021.24750. JAMA Netw Open. 2021. PMID: 34554237 Free PMC article.
-
A Nomogram to Predict Individual Survival of Patients with Liver-Limited Metastases from Gastroenteropancreatic Neuroendocrine Neoplasms: A US Population-Based Cohort Analysis and Chinese Multicenter Cohort Validation Study.Neuroendocrinology. 2022;112(3):263-275. doi: 10.1159/000516812. Epub 2021 Apr 26. Neuroendocrinology. 2022. PMID: 33902058
-
A nomogram for predicting the risk of liver metastasis in non-functional neuroendocrine neoplasms: A population-based study.Eur J Surg Oncol. 2025 May;51(5):109708. doi: 10.1016/j.ejso.2025.109708. Epub 2025 Feb 21. Eur J Surg Oncol. 2025. PMID: 40024114 Review.
-
A New Online Dynamic Nomogram: Construction and Validation of a Predictive Model for Distant Metastasis Risk and Prognosis in Patients with Gastrointestinal Stromal Tumors.J Gastrointest Surg. 2023 Jul;27(7):1429-1444. doi: 10.1007/s11605-023-05706-9. Epub 2023 May 25. J Gastrointest Surg. 2023. PMID: 37231240 Review.
Cited by
-
Development and validation of predictive models for distant metastasis and prognosis of gastroenteropancreatic neuroendocrine neoplasms.Sci Rep. 2025 Mar 19;15(1):9510. doi: 10.1038/s41598-025-92974-x. Sci Rep. 2025. PMID: 40108260 Free PMC article.
-
The Evolving Landscape of GEP-NENs in the Era of Precision Oncology: Molecular Insights into Tumor Heterogeneity.Cancers (Basel). 2025 Jun 21;17(13):2080. doi: 10.3390/cancers17132080. Cancers (Basel). 2025. PMID: 40647381 Free PMC article. Review.
-
Predictive and prognostic nomogram models for liver metastasis in colorectal neuroendocrine neoplasms: a large population study.Front Endocrinol (Lausanne). 2025 Jan 7;15:1488733. doi: 10.3389/fendo.2024.1488733. eCollection 2024. Front Endocrinol (Lausanne). 2025. PMID: 39839478 Free PMC article.
References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical