

Recent advances in rectal cancer treatment - are we on the right track?
- PMID: 38449909
- PMCID: PMC10916366
- DOI: 10.48101/ujms.v129.10537
Recent advances in rectal cancer treatment - are we on the right track?
Abstract
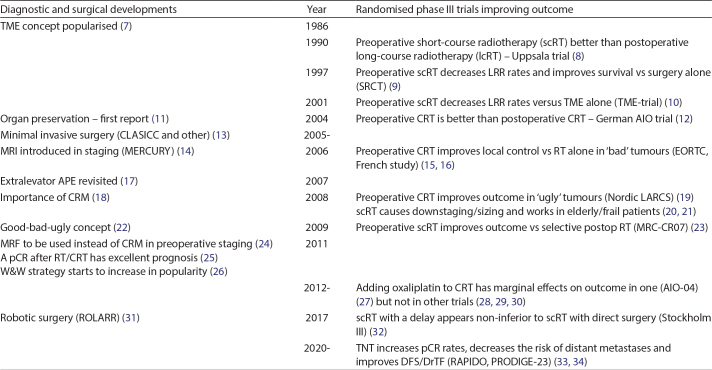
Background: Staging and treatment of rectal cancer have evolved over several decades with considerably fewer locoregional recurrences but no marked improved survival since systemic recurrence risks remain virtually unchanged. This development will briefly be summarised followed by a thorough discussion of two recent developments.
Methods: A systematic approach towards the literature is aimed at focusing on organ preservation and the delivery of all non-surgical treatments prior to surgery or total neoadjuvant treatment (TNT).
Results: Organ preservation, that is to defer surgery if the tumour happens to disappear completely after any pre-treatment given to locally advanced tumours to decrease recurrence risks has increased in popularity and is, if not universally, widely accepted. To give neo-adjuvant treatment to intentionally obtain a clinically complete remission to avoid surgery is practised in some environments but is mostly still experimental. TNT, that is to provide both radiotherapy and chemotherapy aimed at killing microscopic disease in the pelvis or elsewhere has been subject to several trials. Collectively, they show that the chance of achieving a complete response, pathologically or clinically, has approximately doubled, increasing the chance for organ preservation, and the risk of distant metastasis has decreased at least in some trials. The best schedule remains to be established.
Conclusions: To obtain substantial progress and also improve survival, the systemic treatments need to be improved even if preoperative delivery is more effective and better tolerated than postoperative. The locoregional treatment may be further optimised through better risk prediction.
Keywords: Locally advanced rectal cancer; organ preservation; total neoadjuvant treatment; watch and wait.
© 2024 The Author(s). Published by Upsala Medical Society.
Conflict of interest statement
The author reports no conflict of interest.
Figures
References
-
- Storli PE, Dille-Amdam RG, Skjaerseth GH, Gran MV, Myklebust TA, Gronbech JE, et al. Cumulative incidence of first recurrence after curative treatment of stage I-III colorectal cancer. Competing risk analyses of temporal and anatomic patterns. Acta Oncol. 2023;62:1822–30. doi: 10.1080/0284186X.2023.2269644 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources