

Non-ablative Erbium (YAG) and Neodymium (YAG) Laser Treatment for Anal Incontinence and Vaginal Atrophy: A Case Study
- PMID: 38449912
- PMCID: PMC10915698
- DOI: 10.7759/cureus.55542
Non-ablative Erbium (YAG) and Neodymium (YAG) Laser Treatment for Anal Incontinence and Vaginal Atrophy: A Case Study
Abstract
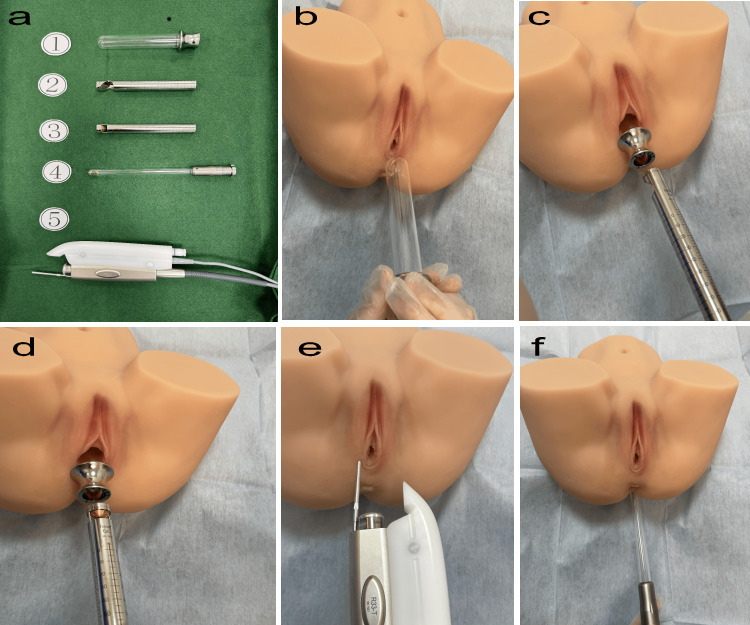
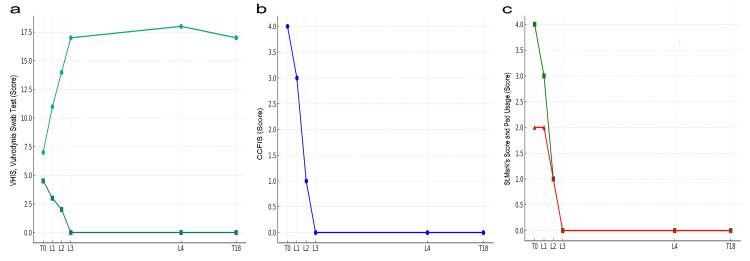
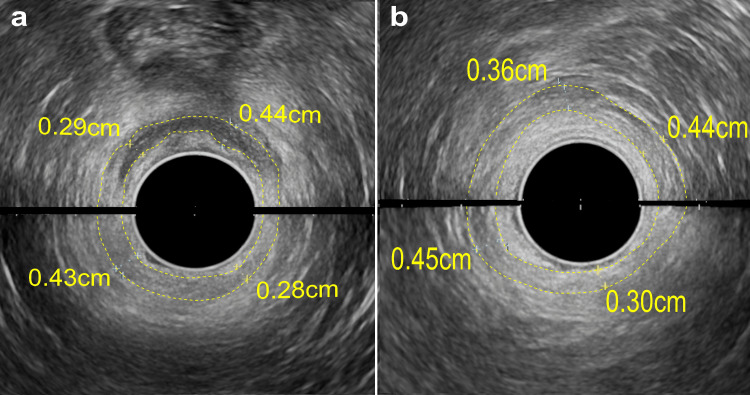
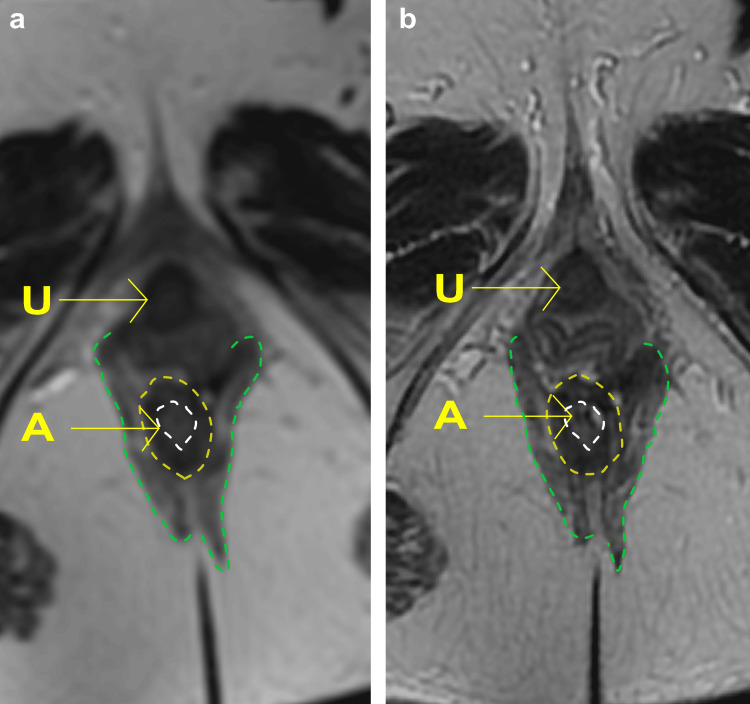
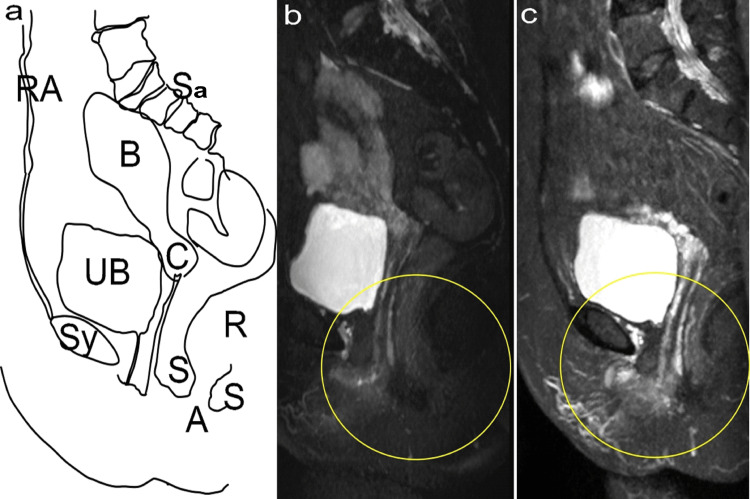
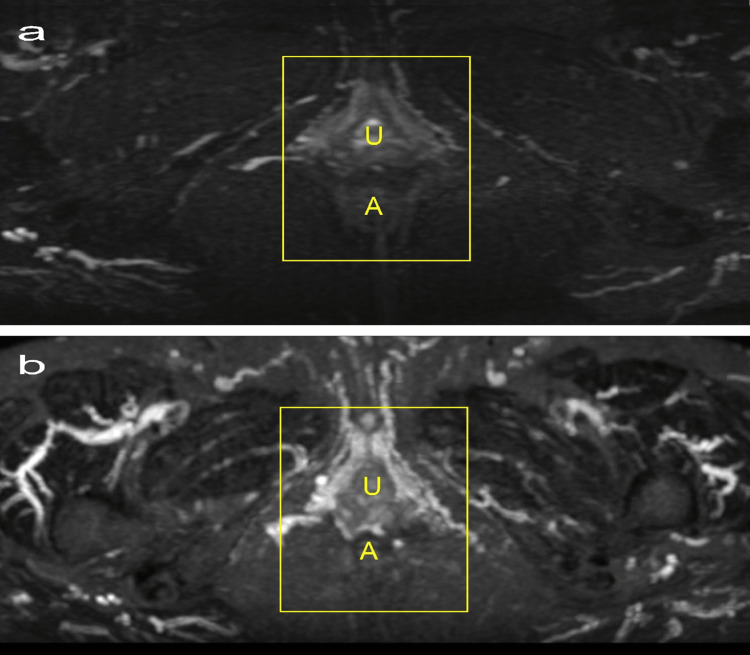
In this case study, a 68-year-old woman with anal incontinence (AI) and vaginal atrophy (VVA), who did not respond to traditional treatments such as pelvic floor exercises or hormone therapy, underwent three sessions of laser treatment using RenovaLase (SP Dynamis; Fotona d.o.o., Ljubljana, Slovenia), which employs non-ablative Erbium:YAG and Neodymium:YAG lasers. Significant improvements were observed in the VVA symptoms, with AI being resolved. The Vaginal Health Index Score increased from 7 points at the initial assessment to 18 points at 12 months after treatment. Similarly, the Cleveland Clinic Florida Fecal Incontinence Score and St. Mark's Incontinence Score, initially at 4 points each, improved to 0 points, indicating resolution of incontinence symptoms. MRI results demonstrated vascular enhancement and growth in the anal sphincter, with the thickness of the internal anal sphincter slightly increasing from initial measurements to a maximum of 0.36 cm, and improvements in resting and squeeze pressures from 42 mmHg to 110 mmHg, respectively. These findings underscore the effectiveness of RenovaLase® laser treatment for VVA and AI symptoms, offering a novel option for pelvic floor health management in postmenopausal women, especially those resistant to the use of artificial devices for anal improvement. In the environment of hormonal decline after menopause, the atrophy of pelvic vessels leads to reduced blood flow. This situation, where a noticeable lack of blood flow occurs during pretreatment of the pelvic vessels, is addressed by laser treatment. This phenomenon has been named "re-canalization." This case suggests the potential of this therapy as an alternative for patients resistant to conventional methods involving the insertion of devices into the anus to improve fecal incontinence. Further research is needed to explore its potential benefits.
Keywords: anal incontinence; cleveland clinic florida fecal incontinence score; erbium:yag; neodymium:yag; st. mark's score; vaginal atrophy; vaginal health index score; vulvodynia swab test.
Copyright © 2024, Okui et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Efficacy and Safety of Combination Therapy With Vaginal and Urethral Erbium-Doped Yttrium-Aluminum-Garnet (Er:YAG) Laser for Overactive Bladder With Urinary Incontinence.Cureus. 2024 Jun 14;16(6):e62363. doi: 10.7759/cureus.62363. eCollection 2024 Jun. Cureus. 2024. PMID: 39006699 Free PMC article.
-
Short-term effects of an erbium/neodymium laser combination in superficial dyspareunia: a pilot study.Climacteric. 2022 Apr;25(2):208-211. doi: 10.1080/13697137.2021.2014809. Epub 2022 Jan 10. Climacteric. 2022. PMID: 35006008
-
Pubovisceral muscle and anal sphincter defects in women with fecal or urinary incontinence after vaginal delivery.Tech Coloproctol. 2019 Feb;23(2):117-128. doi: 10.1007/s10151-018-1895-x. Epub 2018 Nov 26. Tech Coloproctol. 2019. PMID: 30478651
-
The Potential of Non-ablative Erbium (YAG) Laser Treatment for Complications After Midurethral Sling Surgery: A Narrative Review.Cureus. 2024 Apr 17;16(4):e58486. doi: 10.7759/cureus.58486. eCollection 2024 Apr. Cureus. 2024. PMID: 38638175 Free PMC article. Review.
-
Vaginal laser therapy for GSM/VVA: where we stand now - a review by the EUGA Working Group on Laser.Climacteric. 2023 Aug;26(4):336-352. doi: 10.1080/13697137.2023.2225766. Epub 2023 Jul 3. Climacteric. 2023. PMID: 37395104 Review.
Cited by
-
Efficacy of transvaginal erbium laser treatment for vaginal relaxation and its impact on vaginal microenvironment indicators.Am J Transl Res. 2025 Apr 15;17(4):2701-2711. doi: 10.62347/BVZV3932. eCollection 2025. Am J Transl Res. 2025. PMID: 40385007 Free PMC article.
-
Novel Management of Post-laparoscopic Sacrocolpopexy-Associated Overactive Bladder: A Combined Approach of Vaginal Natural Orifice Transluminal Endoscopic Surgery (vNOTES) Mesh Removal and Fotona Laser Therapy.Cureus. 2025 Feb 19;17(2):e79277. doi: 10.7759/cureus.79277. eCollection 2025 Feb. Cureus. 2025. PMID: 40125242 Free PMC article.
-
Pathological Insights on Polypropylene Mesh Complications From Laparoscopic Sacrocolpopexy: A Case Series.Cureus. 2024 Mar 17;16(3):e56354. doi: 10.7759/cureus.56354. eCollection 2024 Mar. Cureus. 2024. PMID: 38501030 Free PMC article.
-
Treatment of Refractory Vesicourethral Anastomosis Pain Following Radical Prostatectomy Using a Combination of Non-ablative Erbium:YAG and Neodymium:YAG Laser Therapy: A Case Report.Cureus. 2024 Jun 24;16(6):e63036. doi: 10.7759/cureus.63036. eCollection 2024 Jun. Cureus. 2024. PMID: 39050360 Free PMC article.
References
-
- An international urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female anorectal dysfunction. Sultan AH, Monga A, Lee J, et al. Int Urogynecol J. 2017;28:5–31. - PubMed
-
- Systematic review of the prevalence of faecal incontinence. Sharma A, Yuan L, Marshall RJ, Merrie AE, Bissett IP. Br J Surg. 2016;103:1589–1597. - PubMed
-
- The American Society of Colon and Rectal Surgeons’ clinical practice guideline for the treatment of fecal incontinence. Paquette IM, Varma MG, Kaiser AM, Steele SR, Rafferty JF. Dis Colon Rectum. 2015;58:623–636. - PubMed
-
- Intravascular imaging during percutaneous coronary intervention: JACC state-of-the-art review. Truesdell AG, Alasnag MA, Kaul P, et al. J Am Coll Cardiol. 2023;81:590–605. - PubMed
Publication types
LinkOut - more resources
Full Text Sources