

Postural impairments in unilateral and bilateral vestibulopathy
- PMID: 38450076
- PMCID: PMC10915085
- DOI: 10.3389/fneur.2024.1324868
Postural impairments in unilateral and bilateral vestibulopathy
Abstract
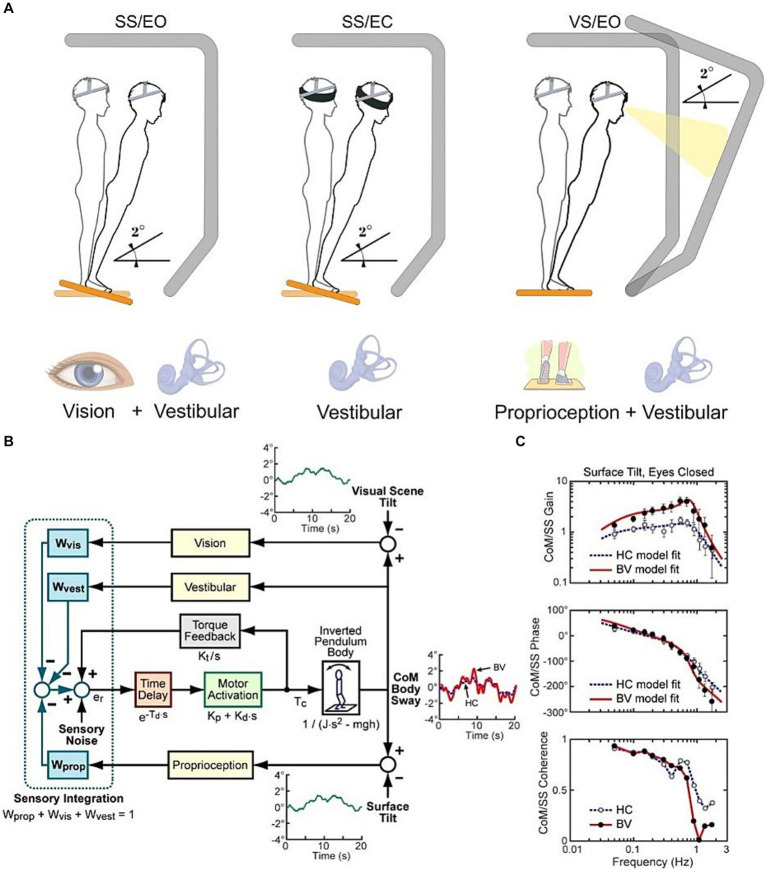
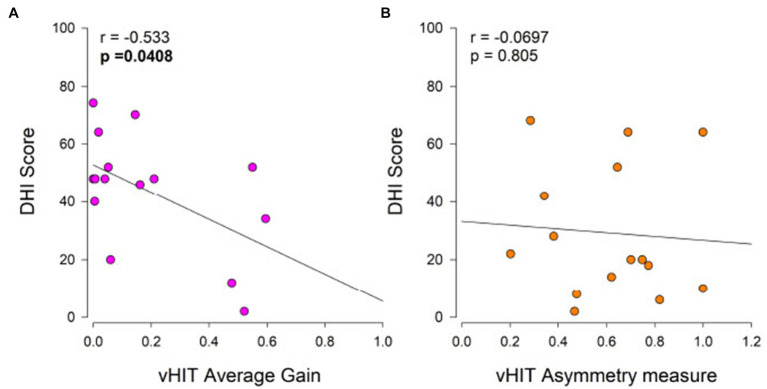
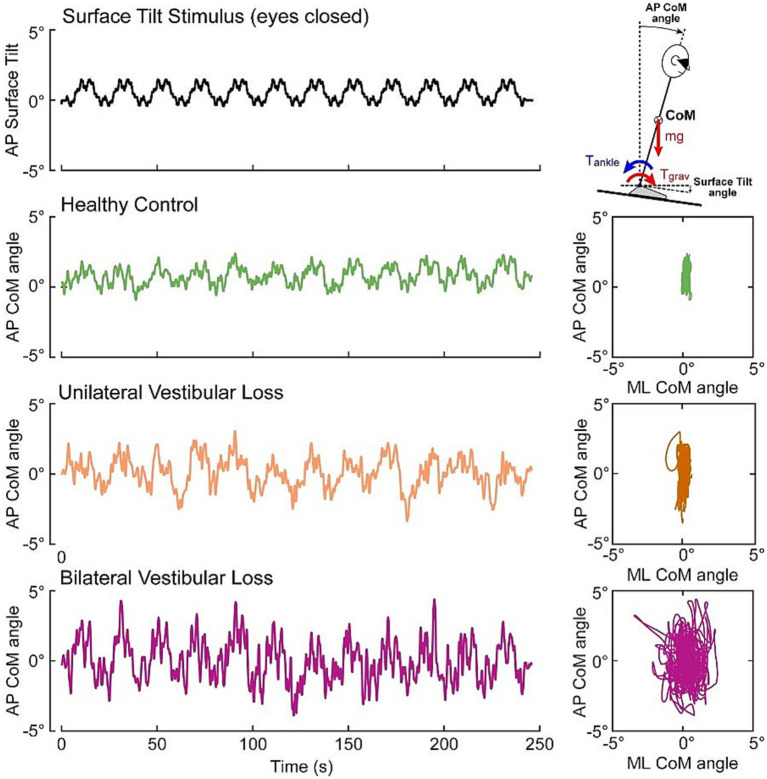
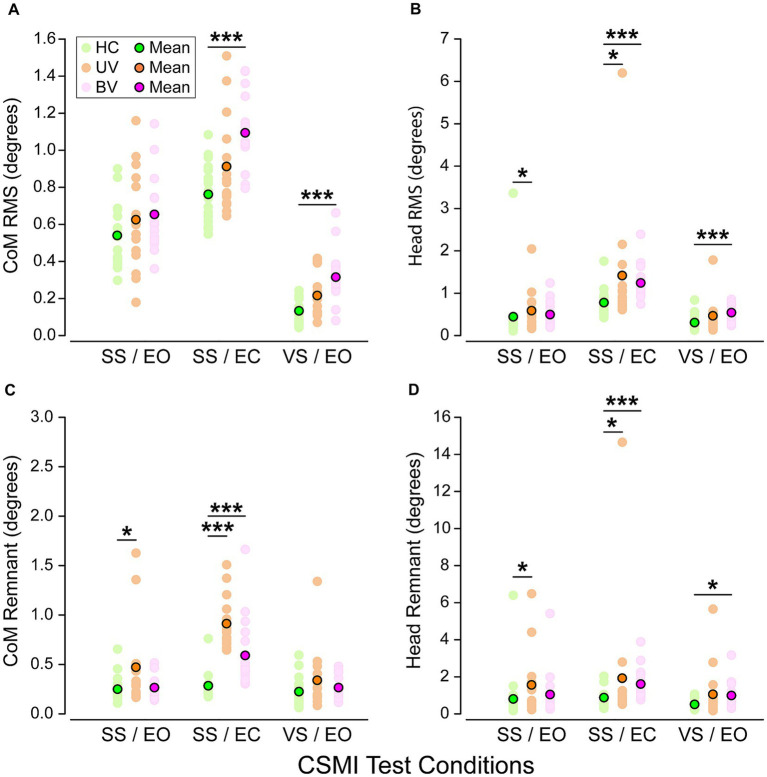
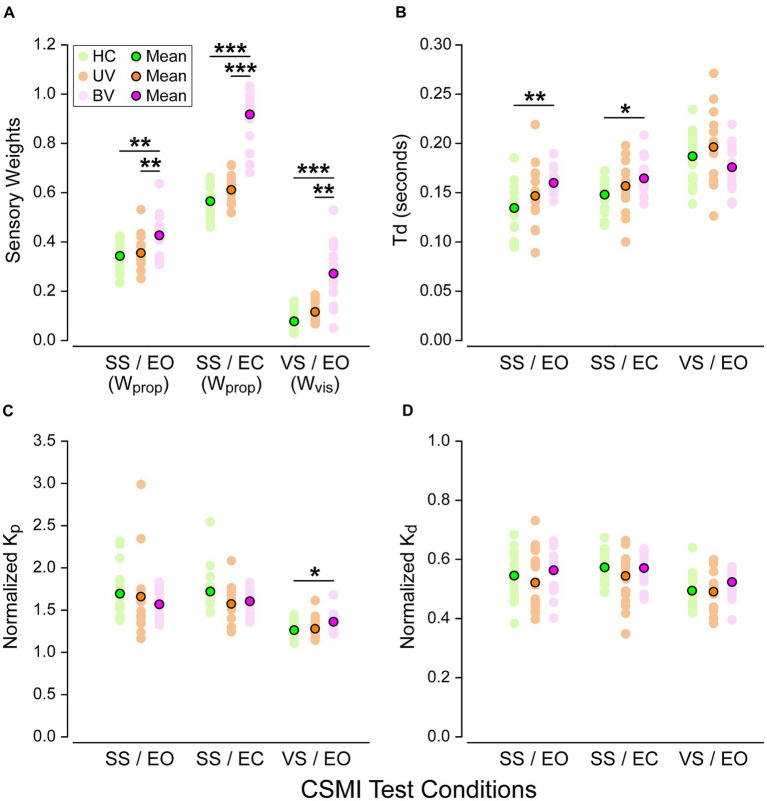
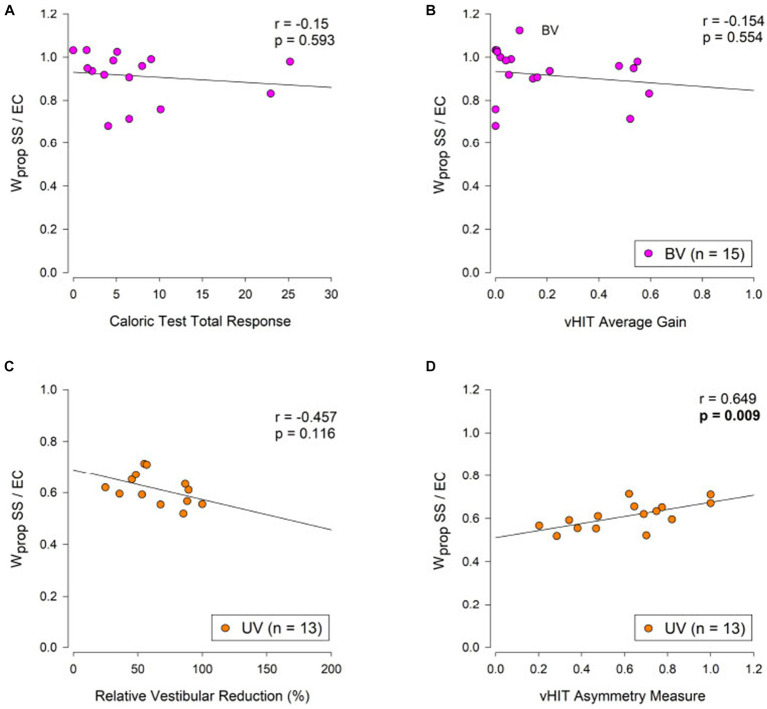
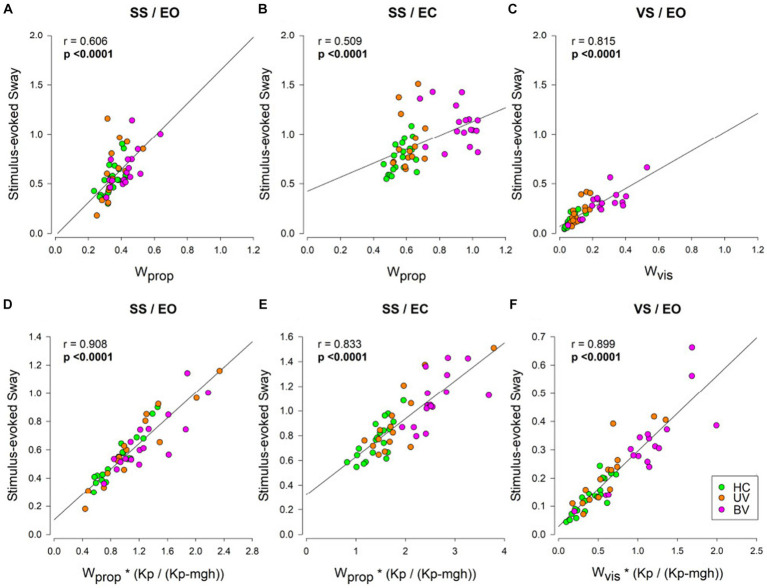
Chronic imbalance is a major complaint of patients suffering from bilateral vestibulopathy (BV) and is often reported by patients with chronic unilateral vestibulopathy (UV), leading to increased risk of falling. We used the Central SensoriMotor Integration (CSMI) test, which evaluates sensory integration, time delay, and motor activation contributions to standing balance control, to determine whether CSMI measures could distinguish between healthy control (HC), UV, and BV subjects and to characterize vestibular, proprioceptive, and visual contributions expressed as sensory weights. We also hypothesized that sensory weight values would be associated with the results of vestibular assessments (vestibulo ocular reflex tests and Dizziness Handicap Inventory scores). Twenty HCs, 15 UVs and 17 BVs performed three CSMI conditions evoking sway in response to pseudorandom (1) surface tilts with eyes open or, (2) surface tilts with eyes closed, and (3) visual surround tilts. Proprioceptive weights were identified in surface tilt conditions and visual weights were identified in the visual tilt condition. BVs relied significantly more on proprioception. There was no overlap in proprioceptive weights between BV and HC subjects and minimal overlap between UV and BV subjects in the eyes-closed surface-tilt condition. Additionally, visual sensory weights were greater in BVs and were similarly able to distinguish BV from HC and UV subjects. We found no significant correlations between sensory weights and the results of vestibular assessments. Sensory weights from CSMI testing could provide a useful measure for diagnosing and for objectively evaluating the effectiveness of rehabilitation efforts and future treatments designed to restore vestibular function such as hair cell regeneration and vestibular implants.
Keywords: balance; bilateral vestibulopathy; posturography; sensory integration; unilateral vestibulopathy; vestibular.
Copyright © 2024 Corre, Cugnot, Boutabla, Cavuscens, Ranieri, van de Berg, Peterka, Guinand and Fornos.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Cullen KE. Chapter 2 - Physiology of central pathways In: Furman JM, Lempert T, editors. Handbook of Clinical Neurology: Elsevier, Amsterdam: (2016). 17–40. - PubMed
LinkOut - more resources
Full Text Sources