

Comparing COVID-19 severity in patients hospitalized for community-associated Delta, BA.1 and BA.4/5 variant infection
- PMID: 38450129
- PMCID: PMC10915065
- DOI: 10.3389/fpubh.2024.1294261
Comparing COVID-19 severity in patients hospitalized for community-associated Delta, BA.1 and BA.4/5 variant infection
Abstract
Background: Despite decreasing COVID-19 disease severity during the Omicron waves, a proportion of patients still require hospitalization and intensive care.
Objective: To compare demographic characteristics, comorbidities, vaccination status, and previous infections in patients hospitalized for community-associated COVID-19 (CAC) in predominantly Delta, Omicron BA.1 and BA.4/5 SARS-CoV-2 waves.
Methods: Data were extracted from three national databases-the National COVID-19 Database, National Vaccination Registry and National Registry of Hospitalizations.
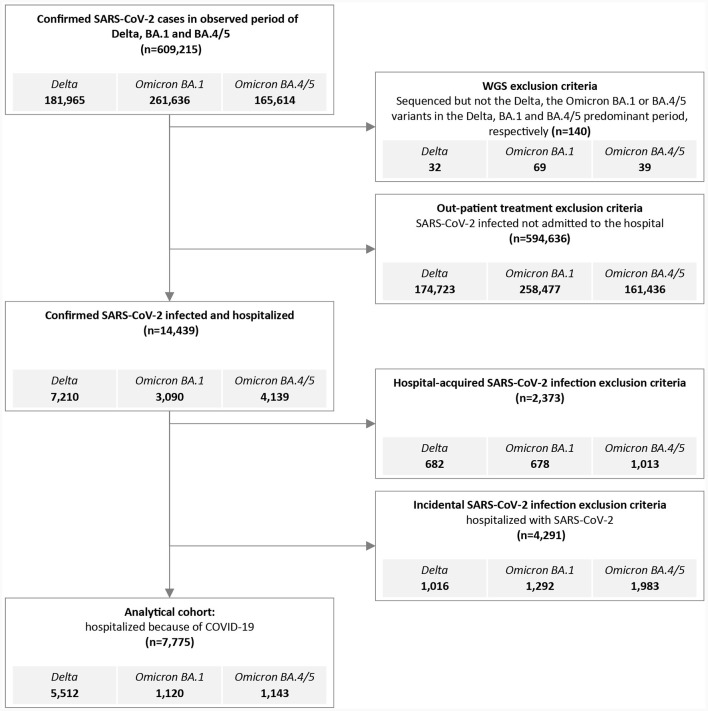
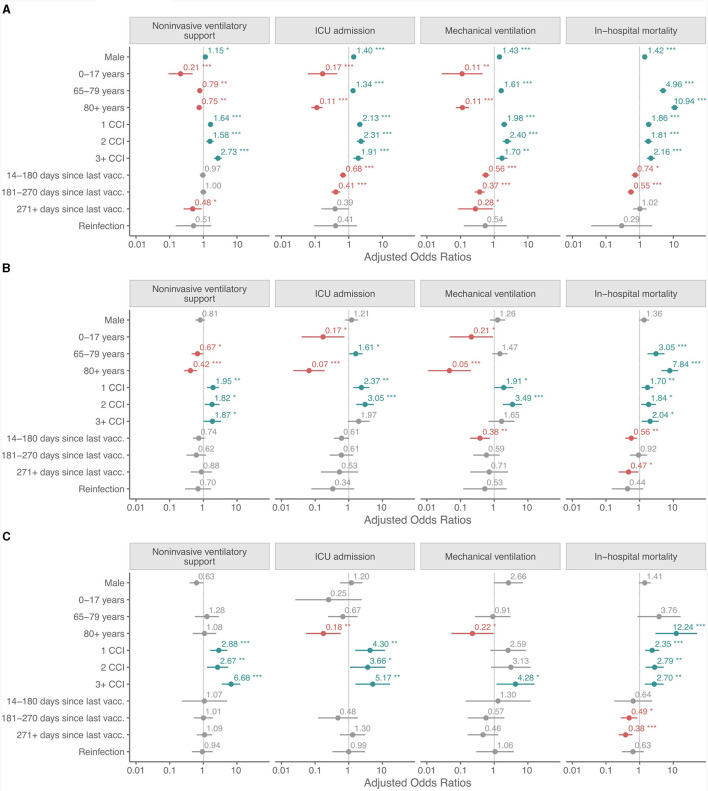
Results: Among the hospitalized CAC patients analyzed in this study, 5,512 were infected with Delta, 1,120 with Omicron BA.1, and 1,143 with the Omicron BA.4/5 variant. The age and sex structure changed from Delta to BA.4/5, with the proportion of women (9.5% increase), children and adolescents (10.4% increase), and octa- and nonagenarians increasing significantly (24.5% increase). Significantly more patients had comorbidities (measured by the Charlson Comorbidity Index), 30.3% in Delta and 43% in BA.4/5 period. The need for non-invasive ventilatory support (NiVS), ICU admission, mechanical ventilation (MV), and in-hospital mortality (IHM) decreased from Delta to Omicron BA.4/5 period for 12.6, 13.5, 11.5, and 6.3%, respectively. Multivariate analysis revealed significantly lower odds for ICU admission (OR 0.68, CI 0.54-0.84, p < 0.001) and IHM (OR 0.74, CI 0.58-0.93, p = 0.011) during the Delta period in patients who had been fully vaccinated or boosted with a COVID-19 vaccine within the previous 6 months. In the BA.1 variant period, patients who had less than 6 months elapsed between the last vaccine dose and SARS-CoV-2 positivity had lower odds for MV (OR 0.38, CI 0.18-0.72, p = 0.005) and IHM (OR 0.56, CI 0.37- 0.83, p = 0.005), but not for NIVS or ICU admission.
Conclusion: The likelihood of developing severe CAC in hospitalized patients was higher in those with the Delta and Omicron BA.1 variant compared to BA.4/5.
Keywords: BA.1; BA.4; BA.5; COVID-19; Delta; Omicron; hospitalization.
Copyright © 2024 Sočan, Mrzel, Prosenc, Korva, Avšič-Županc, Poljak, Lunar and Zupanič.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance - One Hospital, California, July 15-September 23, 2021, and December 21, 2021-January 27, 2022.MMWR Morb Mortal Wkly Rep. 2022 Feb 11;71(6):217-223. doi: 10.15585/mmwr.mm7106e2. MMWR Morb Mortal Wkly Rep. 2022. PMID: 35143466 Free PMC article.
-
Evolution of SARS-CoV-2 variants of concern over a period of Delta and Omicron cocirculation, among patients hospitalized for COVID-19 in an Italian reference hospital: Impact on clinical outcomes.J Med Virol. 2023 Jun;95(6):e28831. doi: 10.1002/jmv.28831. J Med Virol. 2023. PMID: 37246793
-
Protection against symptomatic infection with delta (B.1.617.2) and omicron (B.1.1.529) BA.1 and BA.2 SARS-CoV-2 variants after previous infection and vaccination in adolescents in England, August, 2021-March, 2022: a national, observational, test-negative, case-control study.Lancet Infect Dis. 2023 Apr;23(4):435-444. doi: 10.1016/S1473-3099(22)00729-0. Epub 2022 Nov 24. Lancet Infect Dis. 2023. PMID: 36436536 Free PMC article.
-
Severity and outcomes of Omicron variant of SARS-CoV-2 compared to Delta variant and severity of Omicron sublineages: a systematic review and metanalysis.BMJ Glob Health. 2023 Jul;8(7):e012328. doi: 10.1136/bmjgh-2023-012328. BMJ Glob Health. 2023. PMID: 37419502 Free PMC article.
-
COVID in Pediatric Age: an opinion paper.Rev Esp Quimioter. 2022 Aug;35(4):333-343. doi: 10.37201/req/012.2022. Epub 2022 Mar 15. Rev Esp Quimioter. 2022. PMID: 35287259 Free PMC article. Review.
Cited by
-
Risk factors for mortality in hospitalized COVID-19 patients across five waves in Pakistan.Sci Rep. 2024 Aug 30;14(1):20205. doi: 10.1038/s41598-024-70662-6. Sci Rep. 2024. PMID: 39215007 Free PMC article.
-
Prognostic Value of the Brixia Radiological Score in COVID-19 Patients: A Retrospective Study from Romania.Trop Med Infect Dis. 2025 May 12;10(5):130. doi: 10.3390/tropicalmed10050130. Trop Med Infect Dis. 2025. PMID: 40423360 Free PMC article.
References
-
- Jassat W, Karim SSA, Mudara C, Welch R, Ozougwu L, Groome MJ, et al. . Clinical severity of COVID-19 in patients admitted to hospital during the omicron wave in South Africa: a retrospective observational study. Lancet Glob Health. (2022) 10:e961–9. 10.1016/S2214-109X(22)00114-0 - DOI - PMC - PubMed
-
- Davies MA, Kassanjee R, Rousseau P, Morden E, Johnson L, Solomon W, et al. . Outcomes of laboratory-confirmed SARS-CoV-2 infection in the Omicron-driven fourth wave compared with previous waves in the Western Cape Province, South Africa. Trop Med Int Health. (2022) 27:564–73. 10.1111/tmi.13752 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous