

Isolated Traumatic Subarachnoid Hemorrhage on Head Computed Tomography Scan May Not Be Isolated: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study (TRACK-TBI) Study
- PMID: 38450561
- PMCID: PMC11564841
- DOI: 10.1089/neu.2023.0253
Isolated Traumatic Subarachnoid Hemorrhage on Head Computed Tomography Scan May Not Be Isolated: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study (TRACK-TBI) Study
Abstract
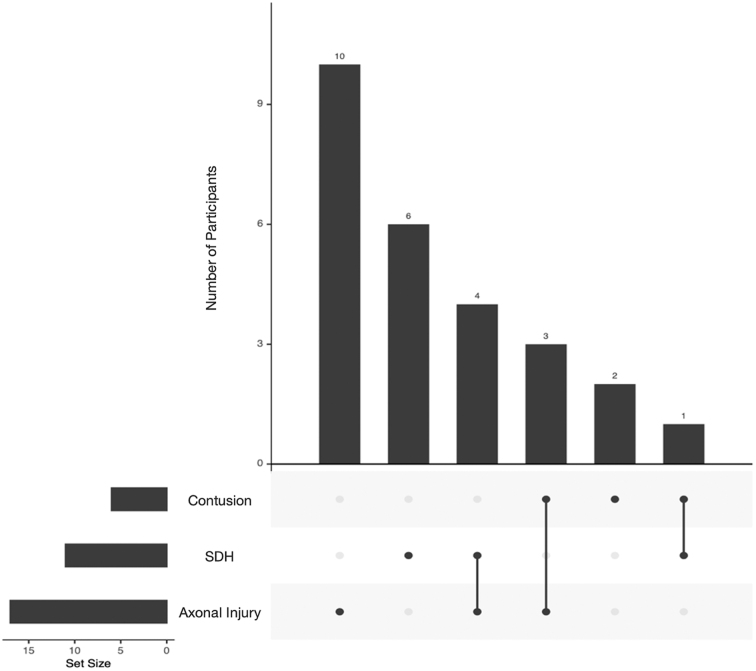
Isolated traumatic subarachnoid hemorrhage (tSAH) after traumatic brain injury (TBI) on head computed tomography (CT) scan is often regarded as a "mild" injury, with reduced need for additional workup. However, tSAH is also a predictor of incomplete recovery and unfavorable outcome. This study aimed to evaluate the characteristics of CT-occult intracranial injuries on brain magnetic resonance imaging (MRI) scan in TBI patients with emergency department (ED) arrival Glasgow Coma Scale (GCS) score 13-15 and isolated tSAH on CT. The prospective, 18-center Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study (TRACK-TBI; enrollment years 2014-2019) enrolled participants who presented to the ED and received a clinically-indicated head CT within 24 h of TBI. A subset of TRACK-TBI participants underwent venipuncture within 24 h for plasma glial fibrillary acidic protein (GFAP) analysis, and research MRI at 2-weeks post-injury. In the current study, TRACK-TBI participants age ≥17 years with ED arrival GCS 13-15, isolated tSAH on initial head CT, plasma GFAP level, and 2-week MRI data were analyzed. In 57 participants, median age was 46.0 years [quartile 1 to 3 (Q1-Q3): 34-57] and 52.6% were male. At ED disposition, 12.3% were discharged home, 61.4% were admitted to hospital ward, and 26.3% to intensive care unit. MRI identified CT-occult traumatic intracranial lesions in 45.6% (26 of 57 participants; one additional lesion type: 31.6%; 2 additional lesion types: 14.0%); of these 26 participants with CT-occult intracranial lesions, 65.4% had axonal injury, 42.3% had subdural hematoma, and 23.1% had intracerebral contusion. GFAP levels were higher in participants with CT-occult MRI lesions compared with without (median: 630.6 pg/mL, Q1-Q3: [172.4-941.2] vs. 226.4 [105.8-436.1], p = 0.049), and were associated with axonal injury (no: median 226.7 pg/mL [109.6-435.1], yes: 828.6 pg/mL [204.0-1194.3], p = 0.009). Our results indicate that isolated tSAH on head CT is often not the sole intracranial traumatic injury in GCS 13-15 TBI. Forty-six percent of patients in our cohort (26 of 57 participants) had additional CT-occult traumatic lesions on MRI. Plasma GFAP may be an important biomarker for the identification of additional CT-occult injuries, including axonal injury. These findings should be interpreted cautiously given our small sample size and await validation from larger studies.
Keywords: diagnosis; glial fibrillary acidic protein; medical decision-making; neuroimaging; traumatic brain injury; traumatic subarachnoid hemorrhage.
Figures


References
-
- Centers for Disease Control and Prevention. TBI Data. 2022. Available from: https://www.cdc.gov/traumaticbraininjury/data/index.html [Last accessed: April 6, 2023].
-
- Nelson LD, Temkin NR, Dikmen S, et al. Recovery after mild traumatic brain injury in patients presenting to US level I trauma centers: a Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study. JAMA Neurol 2019;76(9):1049–1059; doi: 10.1001/jamaneurol.2019.1313 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
