

Multi-Energy Low-Kiloelectron Volt versus Single-Energy Low-Kilovolt Images for Endoleak Detection at CT Angiography of the Aorta
- PMID: 38451189
- PMCID: PMC11056760
- DOI: 10.1148/ryct.230217
Multi-Energy Low-Kiloelectron Volt versus Single-Energy Low-Kilovolt Images for Endoleak Detection at CT Angiography of the Aorta
Abstract
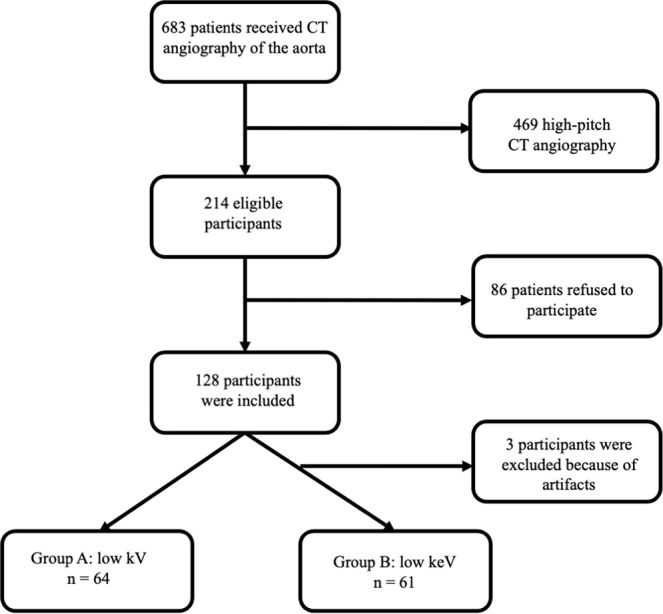
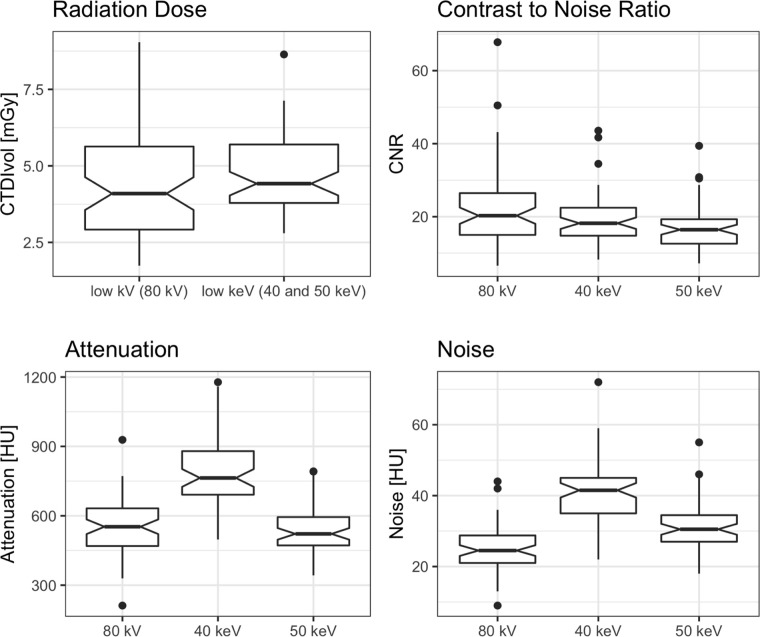
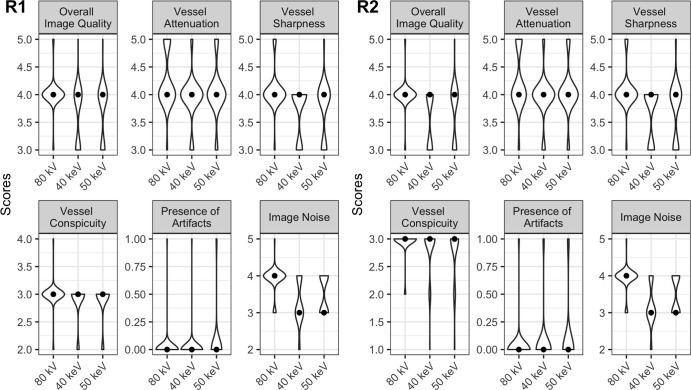
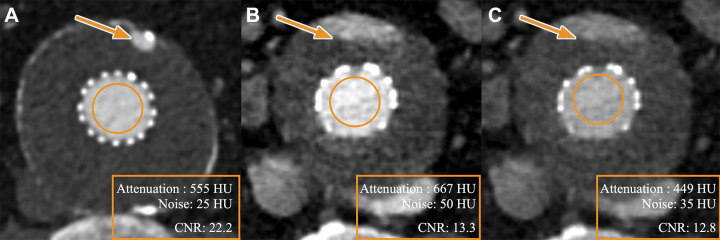
Purpose To compare image quality, diagnostic performance, and conspicuity between single-energy and multi-energy images for endoleak detection at CT angiography (CTA) after endovascular aortic repair (EVAR). Materials and Methods In this single-center prospective randomized controlled trial, individuals undergoing CTA after EVAR between August 2020 and May 2022 were allocated to imaging using either low-kilovolt single-energy images (SEI; 80 kV, group A) or low-kiloelectron volt virtual monoenergetic images (VMI) at 40 and 50 keV from multi-energy CT (80/Sn150 kV, group B). Scan protocols were dose matched (volume CT dose index: mean, 4.5 mGy ± 1.8 [SD] vs 4.7 mGy ± 1.3, P = .41). Contrast-to-noise ratio (CNR) was measured. Two expert radiologists established the reference standard for the presence of endoleaks. Detection and conspicuity of endoleaks and subjective image quality were assessed by two different blinded radiologists. Interreader agreement was calculated. Nonparametric statistical tests were used. Results A total of 125 participants (mean age, 76 years ± 8; 103 men) were allocated to groups A (n = 64) and B (n = 61). CNR was significantly lower for 40-keV VMI (mean, 19.1; P = .048) and 50-keV VMI (mean, 16.8; P < .001) as compared with SEI (mean, 22.2). In total, 45 endoleaks were present (A: 23 vs B: 22). Sensitivity for endoleak detection was higher for SEI (82.6%, 19 of 23; P = .88) and 50-keV VMI (81.8%, 18 of 22; P = .90) as compared with 40-keV VMI (77.3%, 17 of 22). Specificity was comparable among groups (SEI: 92.7%, 38 of 41; both VMI energies: 92.3%, 35 of 38; P = .99), with an interreader agreement of 1. Conspicuity of endoleaks was comparable between SEI (median, 2.99) and VMI (both energies: median, 2.87; P = .04). Overall subjective image quality was rated significantly higher for SEI (median, 4 [IQR, 4-4) as compared with 40 and 50 keV (both energies: median, 4 [IQR, 3-4]; P < .001). Conclusion SEI demonstrated higher image quality and comparable diagnostic accuracy as compared with 50-keV VMI for endoleak detection at CTA after EVAR. Keywords: Aneurysms, CT, CT Angiography, Vascular, Aorta, Technology Assessment, Multidetector CT, Abdominal Aortic Aneurysms, Endoleaks, Perigraft Leak Supplemental material is available for this article. © RSNA, 2024.
Keywords: Abdominal Aortic Aneurysms; Aneurysms; Aorta; CT; CT Angiography; Endoleaks; Multidetector CT; Perigraft Leak; Technology Assessment; Vascular.
Conflict of interest statement
Figures
References
-
- Bulder RMA , Bastiaannet E , Hamming JF , Lindeman JHN . Meta-analysis of long-term survival after elective endovascular or open repair of abdominal aortic aneurysm . Br J Surg 2019. ; 106 ( 5 ): 523 – 533 . - PubMed
-
- Cassagnes L , Pérignon R , Amokrane F , et al . Aortic stent-grafts: Endoleak surveillance . Diagn Interv Imaging 2016. ; 97 ( 1 ): 19 – 27 . - PubMed
-
- Chaikof EL , Dalman RL , Eskandari MK , et al . The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm . J Vasc Surg 2018. ; 67 ( 1 ): 2 – 77.e2 . - PubMed
-
- Smith T , Quencer KB . Best practice guidelines: imaging surveillance after endovascular aneurysm repair . AJR Am J Roentgenol 2020. ; 214 ( 5 ): 1165 – 1174 . - PubMed
-
- Higashigaito K , Schmid T , Puippe G , et al . CT angiography of the aorta: prospective evaluation of individualized low-volume contrast media protocols . Radiology 2016. ; 280 ( 3 ): 960 – 968 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
