

Optimizing periprosthetic fracture management and in-hospital outcome: insights from the PIPPAS multicentric study of 1387 cases in Spain
- PMID: 38451303
- PMCID: PMC10920552
- DOI: 10.1186/s10195-024-00746-6
Optimizing periprosthetic fracture management and in-hospital outcome: insights from the PIPPAS multicentric study of 1387 cases in Spain
Abstract
Background: The incidence of all periprosthetic fractures (PPF), which require complex surgical treatment associated with high morbidity and mortality, is predicted to increase. The evolving surgical management has created a knowledge gap regarding its impact on immediate outcomes. This study aimed to describe current management strategies for PPF and their repercussions for in-hospital outcomes as well as to evaluate their implications for the community.
Methods: PIPPAS (Peri-Implant PeriProsthetic Survival Analysis) was a prospective multicentre observational study of 1387 PPF performed during 2021. Descriptive statistics summarized the epidemiology, fracture characteristics, management, and immediate outcomes. A mixed-effects logistic regression model was employed to evaluate potential predictors of in-hospital mortality, complications, discharge status, and weight-bearing restrictions.
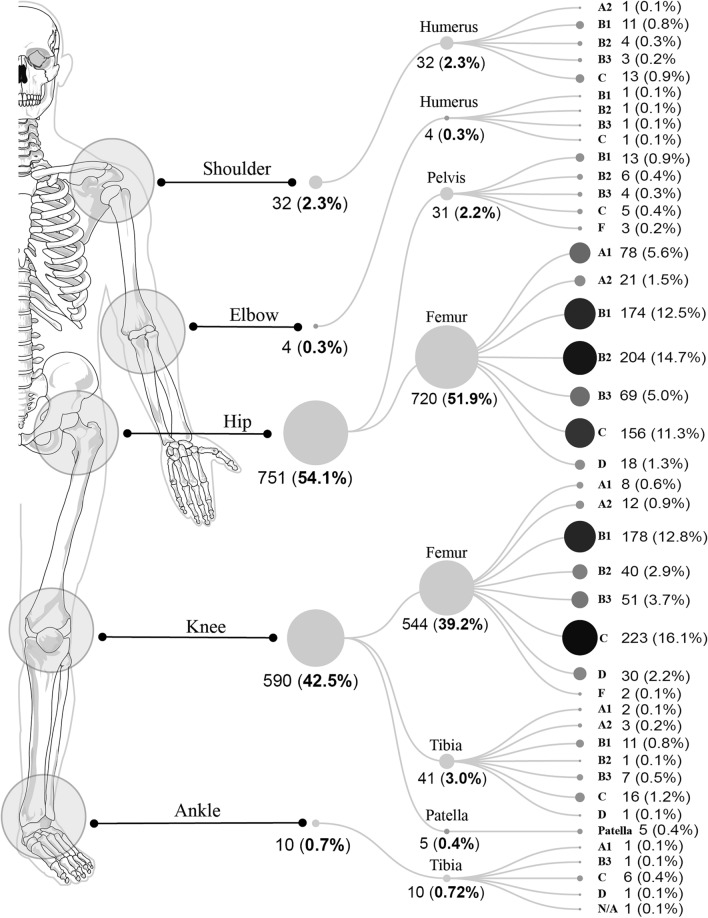
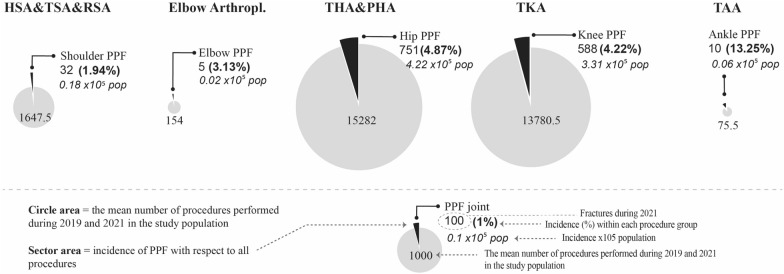
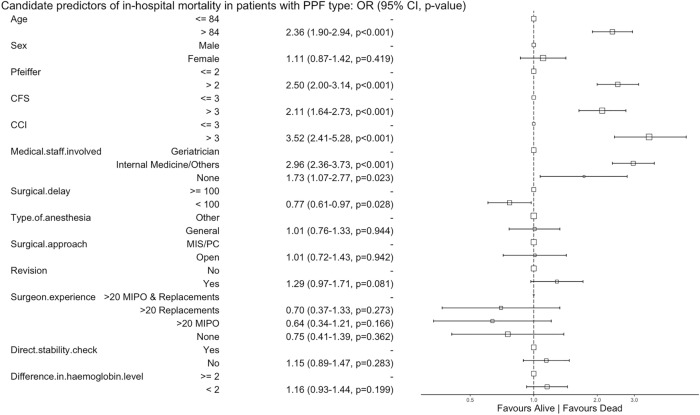
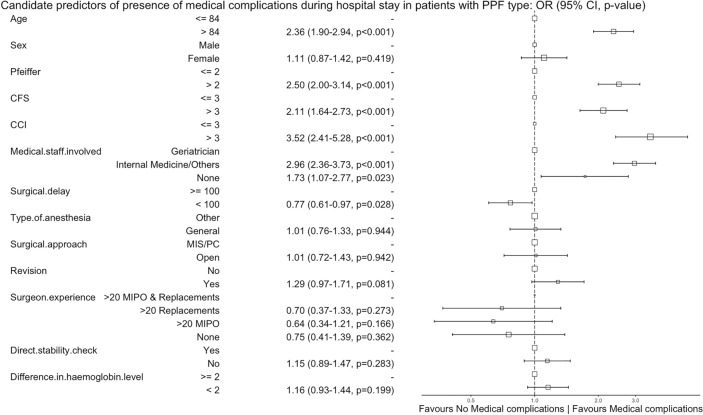
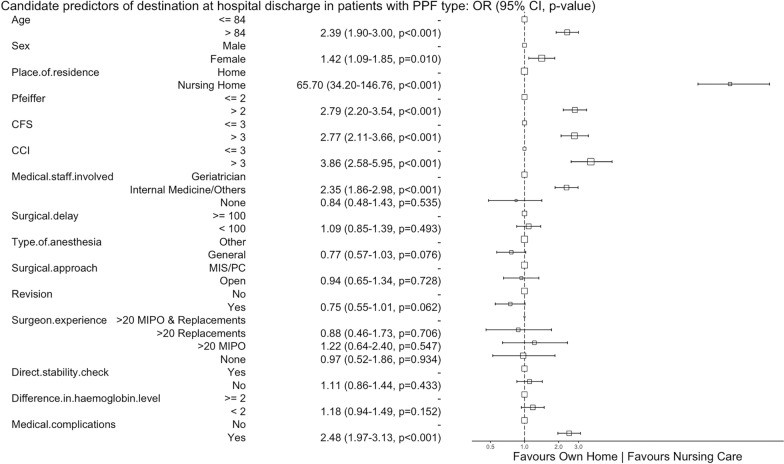
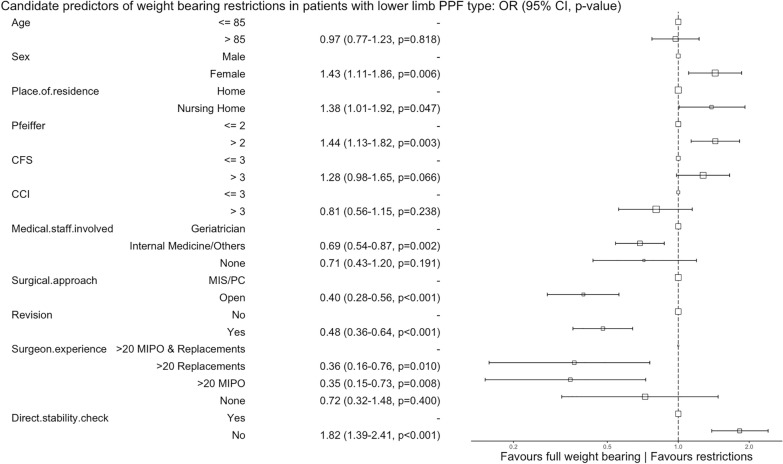
Results: The study encompassed 32 (2.3%) shoulder, 4 (0.3%) elbow, 751 (54.1%) hip, 590 (42.5%) knee, and 10 (0.7%) ankle PPF. Patients were older (median 84 years, IQR 77-89), frail [median clinical frailty scale (CFS) 5, IQR 3-6], presented at least one comorbidity [median Charlson comorbidity index (CCI) 5, IQR 4-7], were community dwelling (81.8%), and had outdoor ambulation ability (65.6%). Femoral knee PPF were most frequently associated with uncemented femoral components, while femoral hip PPF occurred equally in cemented and uncemented stems. Patients were managed surgically (82%), with co-management (73.9%), through open approaches (85.9%) after almost 4 days (IQR, 51.9-153.6 h), with prosthesis revision performed in 33.8% of femoral hip PPF and 6.5% of femoral knee PPF. For half of the patients, the discharge instructions mandated weight-bearing restrictions. In-hospital mortality rates were 5.2% for all PPF and 6.2% for femoral hip PPF. Frailty, age > 84 years, mild cognitive impairment, CFS > 3, CCI > 3, and non-geriatric involvement were candidate predictors for in-hospital mortality, medical complications, and discharge to a nursing care facility. Management involving revision arthroplasty by experienced surgeons favoured full weight-bearing, while an open surgical approach favoured weight-bearing restrictions.
Conclusions: Current arthroplasty fixation check and revision rates deviate from established guidelines, yet full weight-bearing is favoured. A surgical delay of over 100 h and a lack of geriatric co-management were related to in-hospital mortality and medical complications. This study recommends judicious hypoaggressive approaches. Addressing complications and individualizing the surgical strategy can lead to enhanced functional outcomes, alleviating the economic and social burdens upon hospital discharge. Level of Evidence Level IV case series.
Trial registration: registered at ClinicalTrials.gov (NCT04663893), protocol ID: PI 20-2041.
Keywords: Epidemiology; Fracture fixation; Frailty; Geriatric co-management; Incidence; Management; Mortality; Outcome; Periprosthetic fracture; Replacement.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Khan T, Middleton R, Alvand A, Manktelow ARJ, Scammell BE, Ollivere BJ. High mortality following revision hip arthroplasty for periprosthetic femoral fracture: a cohort study using national joint registry data. Bone Jt J. 2020;102(B12):1670–1674. doi: 10.1302/0301-620X.102B12.BJJ-2020-0367.R1. - DOI - PubMed
-
- Slullitel PA, Garcia-Barreiro GG, Oñativia JI, Zanotti G, Comba F, Piccaluga F, et al. Selected Vancouver B2 periprosthetic femoral fractures around cemented polished femoral components can be safely treated with osteosynthesis. Bone Jt J. 2021;103(B7):1222–1230. doi: 10.1302/0301-620X.103B7.BJJ-2020-1809.R1. - DOI - PubMed
-
- Ruchholtz S, El-Zayat B, Kreslo D, Bücking B, Lewan U, Krüger A et al (2013) Less invasive polyaxial locking plate fixation in periprosthetic and peri-implant fractures of the femur—a prospective study of 41 patients. Injury 44(2):239–248 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
