

Success Predictors of Endoscopic Sleeve Gastroplasty
- PMID: 38451369
- PMCID: PMC11031450
- DOI: 10.1007/s11695-024-07109-4
Success Predictors of Endoscopic Sleeve Gastroplasty
Abstract
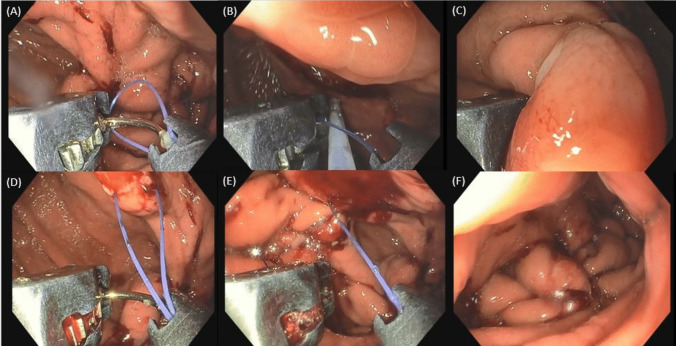
Objective: Endoscopic sleeve gastroplasty (ESG) is a minimally invasive procedure that proved to be safe and effective in obesity treatment. However, not all subjects respond to treatment in the same way, and, with a view to personalized care, it is essential to identify predictors of success or failure.
Methods: A retrospective 2-year followed-up cohort of ESG subjects was analyzed to investigate the presence of any baseline or early indicators of long-term optimal or suboptimal ESG outcomes.
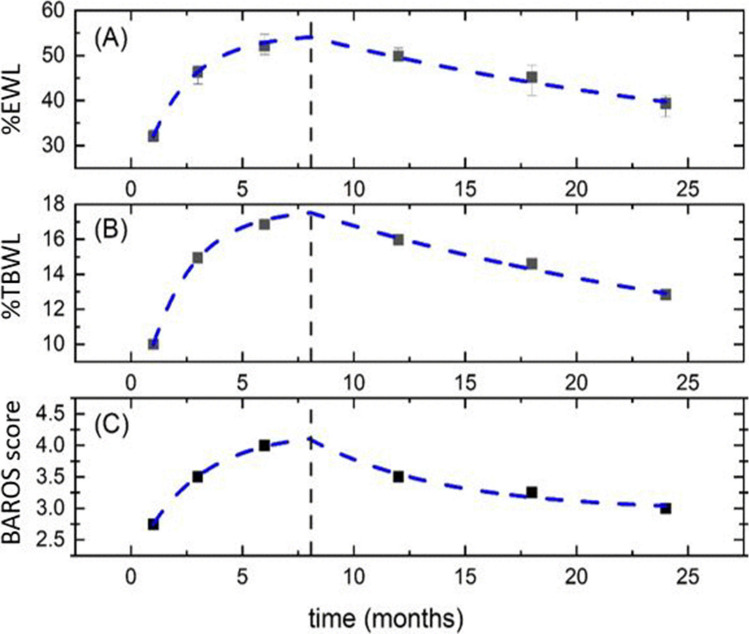
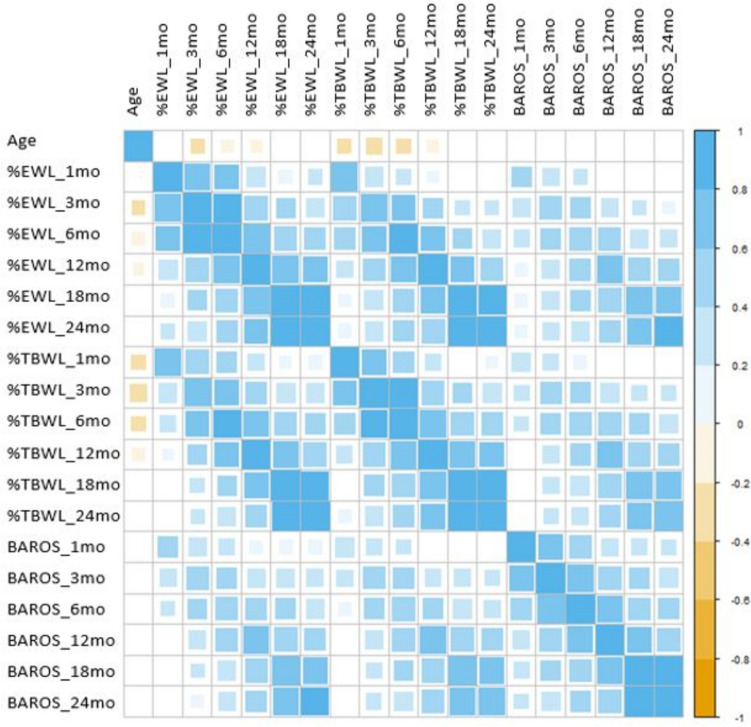
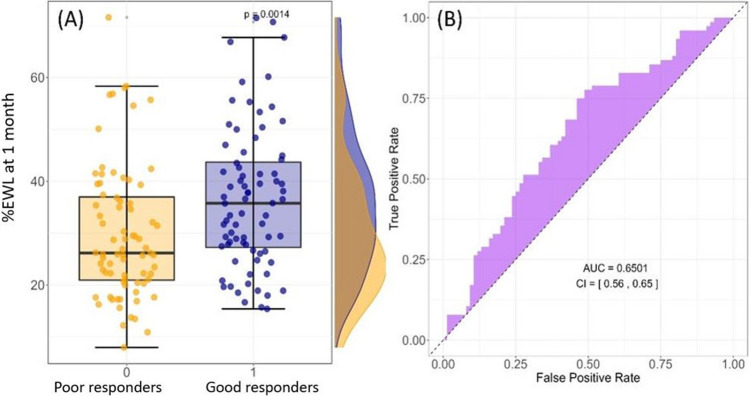
Results: A total of 315 subjects (73% women) were included, with 73% of patients exhibiting an Excess weight loss percentage (%EWL) >25% at the 24 months. Neither demographic parameters (age and sex), smoking habits, and menopause in women nor the presence of comorbidities proved potential predictive value. Interestingly, the %EWL at 1 month after ESG was the strongest predictor of 24-month therapeutic success. Subsequently, we estimated an "early threshold for success" for 1 month-%EWL by employing Youden's index method.
Conclusions: ESG is a safe and effective bariatric treatment that can be offered to a wide range of subjects. Early weight loss seems to impact long-term ESG results significantly and may allow proper early post-operative care optimization.
Keywords: ESG; Endoscopic sleeve gastroplasty; Obesity; Predictors.
© 2024. The Author(s).
Conflict of interest statement
Ivo Boskoski is a consultant for Apollo Endosurgery, Boston Scientific, Nitinotes, Pentax, Cook Medical, Microtech, ERBE, and Endo Tools Therapeutics S.A. Cristiano Spada is a consultant for Medtronic and AnX Robotics and received speaker’s fees from Olympus and Pentax. All the other authors have nothing to declare.
Figures
References
-
- World Health Organization. Obesity and overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 30 Dec 2023.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
