

Efficacy and Safety of Radiotherapy Plus Relugolix in Men With Localized or Advanced Prostate Cancer
- PMID: 38451492
- PMCID: PMC10921349
- DOI: 10.1001/jamaoncol.2023.7279
Efficacy and Safety of Radiotherapy Plus Relugolix in Men With Localized or Advanced Prostate Cancer
Abstract
Importance: Combination androgen deprivation therapy (ADT) with radiotherapy is commonly used for patients with localized and advanced prostate cancer.
Objective: To assess the efficacy and safety of the oral gonadotropin-releasing hormone antagonist relugolix with radiotherapy for treating prostate cancer.
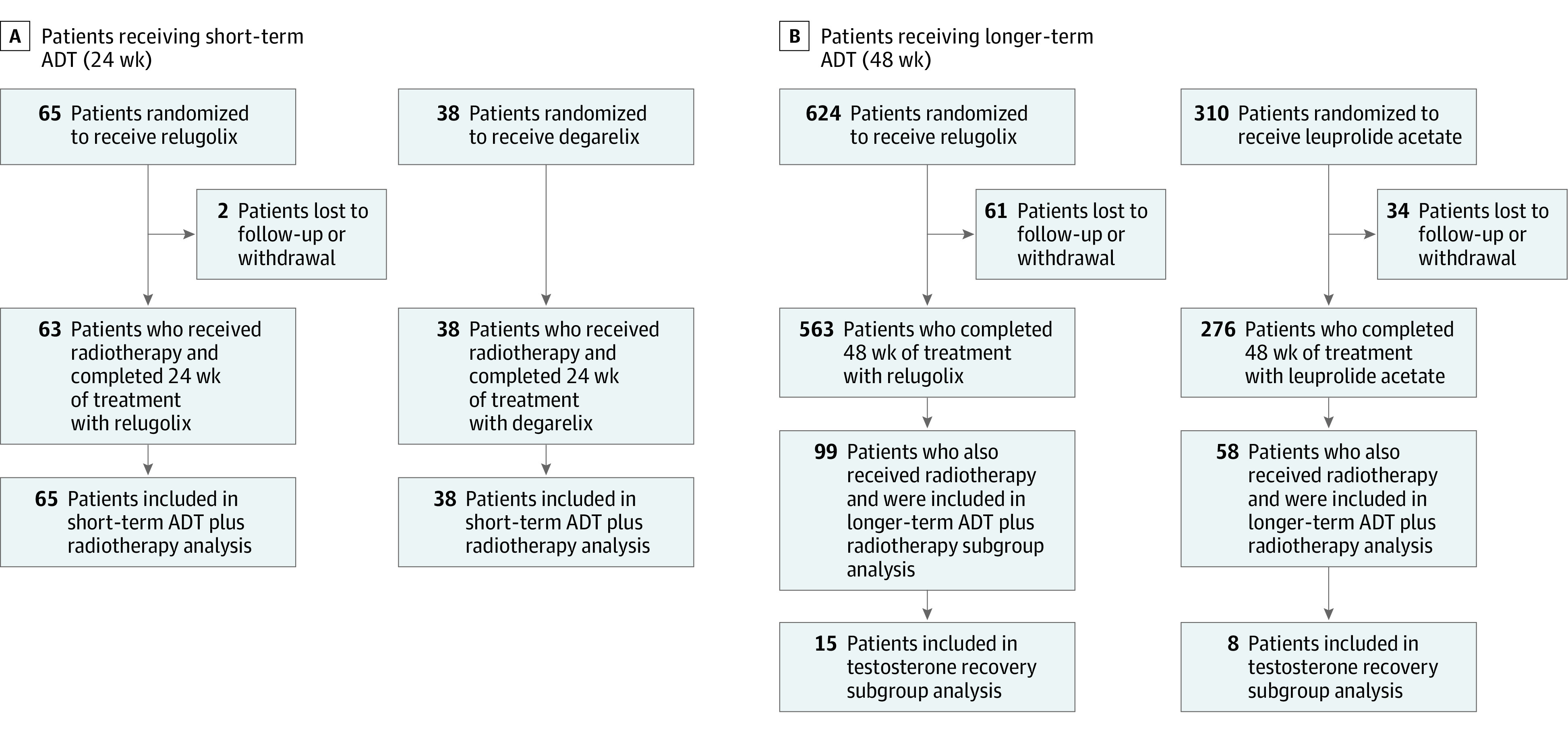
Design, setting, and participants: This multicenter post hoc analysis of patients with localized and advanced prostate cancer receiving radiotherapy in 2 randomized clinical trials (a phase 2 trial of relugolix vs degarelix, and a subset of the phase 3 HERO trial of relugolix vs leuprolide acetate) included men who were receiving radiotherapy and short-term (24 weeks) ADT (n = 103) from 2014 to 2015 and men receiving radiotherapy and longer-term (48 weeks) ADT (n = 157) from 2017 to 2019. The data were analyzed in November 2022.
Interventions: Patients receiving short-term ADT received relugolix, 120 mg, orally once daily (320-mg loading dose) or degarelix, 80 mg, 4-week depot (240-mg loading dose) for 24 weeks with 12 weeks of follow-up. Patients receiving longer-term ADT received relugolix, 120 mg, orally once daily (360-mg loading dose) or leuprolide acetate injections every 12 weeks for 48 weeks, with up to 90 days of follow-up.
Main outcomes and measures: Castration rate (testosterone level <50 ng/dL [to convert to nmol/L, multiply by 0.0347) at all scheduled visits between weeks 5 and 25 for patients receiving short-term ADT and weeks 5 and 49 for patients receiving longer-term ADT.
Results: Of 260 patients (38 Asian [14.6%], 23 Black or African American [8.8%], 21 Hispanic [8.1%], and 188 White [72.3%] individuals), 164 (63.1%) received relugolix. Relugolix achieved castration rates of 95% (95% CI, 87.1%-99.0%) and 97% (95% CI, 90.6%-99.0%) among patients receiving short-term and longer-term ADT, respectively. Twelve weeks post-short-term relugolix, 34 (52%) achieved testosterone levels to baseline or more than 280 ng/dL. Ninety days post longer-term ADT, mean (SD) testosterone levels were 310.5 (122.4) (106.7) ng/dL (relugolix; n = 15) vs 53.0 ng/dL (leuprolide acetate; n = 8) among the subset assessed for testosterone recovery. Castration resistance-free survival was not statistically different between the relugolix and leuprolide acetate cohorts (hazard ratio, 0.97; 95% CI, 0.35-2.72; P = .62). Adverse events grade 3 or greater for short-term or longer-term relugolix (headache, hypertension, and atrial fibrillation) were uncommon (less than 5%).
Conclusions and relevance: The results of these 2 randomized clinical trials suggest that relugolix rapidly achieves sustained castration in patients with localized and advanced prostate cancer receiving radiotherapy. No new safety concerns were identified when relugolix was used with radiotherapy.
Conflict of interest statement
Figures


References
-
- National Comprehensive Cancer Network . Clinical practice guidelines in oncology: prostate cancer, version 2. Accessed October 27, 2022. https://jnccn.org/view/journals/jnccn/17/5/article-p479.xml
-
- Parker CC, James ND, Brawley CD, et al. ; Systemic Therapy for Advanced or Metastatic Prostate cancer: Evaluation of Drug Efficacy Investigators . Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018;392(10162):2353-2366. doi:10.1016/S0140-6736(18)32486-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
