

Drug Efficacy in the Treatment of Antipsychotic-Induced Akathisia: A Systematic Review and Network Meta-Analysis
- PMID: 38451521
- PMCID: PMC10921255
- DOI: 10.1001/jamanetworkopen.2024.1527
Drug Efficacy in the Treatment of Antipsychotic-Induced Akathisia: A Systematic Review and Network Meta-Analysis
Abstract
Importance: Antipsychotic-induced akathisia (AIA) occurs in 14% to 35% of patients treated with antipsychotics and is associated with increased suicide and decreased adherence in patients with schizophrenia. However, no comprehensive review and network meta-analysis has been conducted to compare the efficacy of treatments for AIA.
Objective: To compare the efficacy associated with AIA treatments.
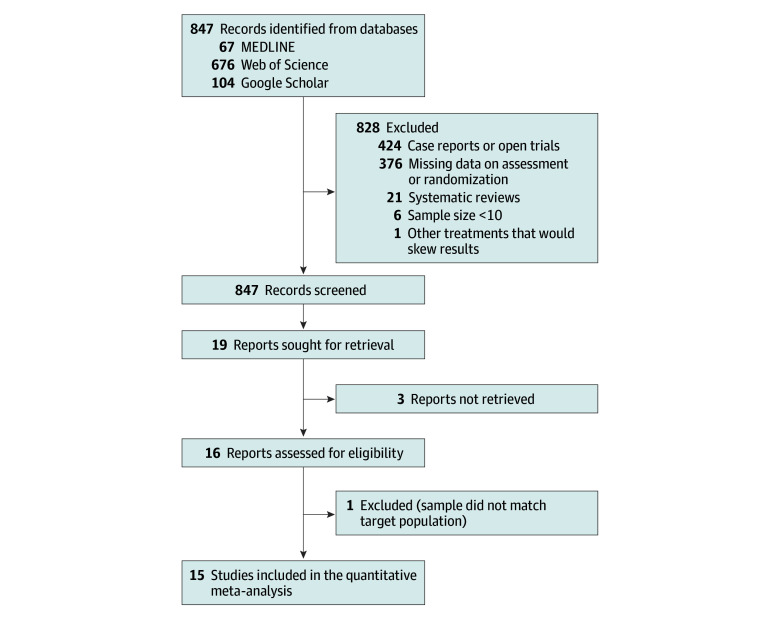
Data sources: Three databases (MEDLINE, Web of Science, and Google Scholar) were systematically searched by multiple researchers for double-blind randomized clinical trials (RCTs) comparing active drugs for the treatment of AIA with placebo or another treatment between May 30 and June 18, 2023.
Study selection: Selected studies were RCTs that compared adjunctive drugs for AIA vs placebo or adjunctive treatment in patients treated with antipsychotics fulfilling the criteria for akathisia, RCTs with sample size of 10 patients or more, only trials in which no additional drugs were administered during the study, and RCTs that used a validated akathisia score. Trials with missing data for the main outcome (akathisia score at the end points) were excluded.
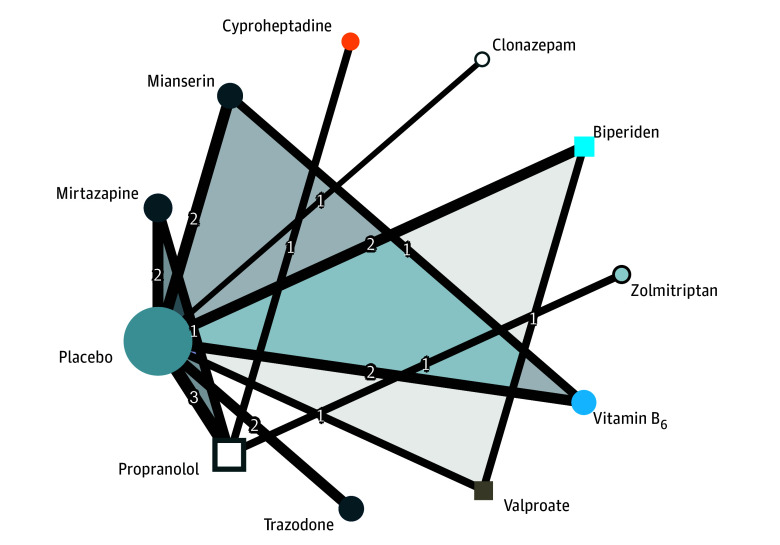
Data extraction and synthesis: Data extraction and synthesis were performed, estimating standardized mean differences (SMDs) through pairwise and network meta-analysis with a random-effects model. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was followed.
Main outcomes and measures: The primary outcome was the severity of akathisia measured by a validated scale at the last available end point.
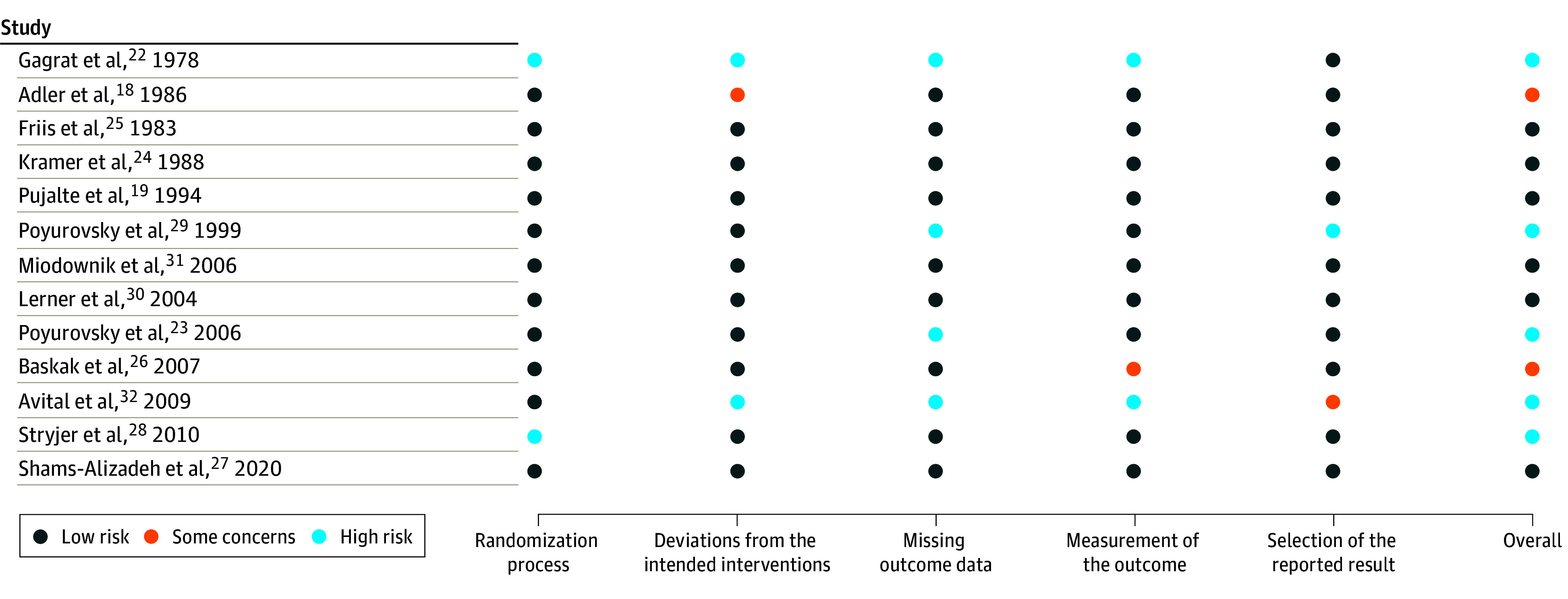
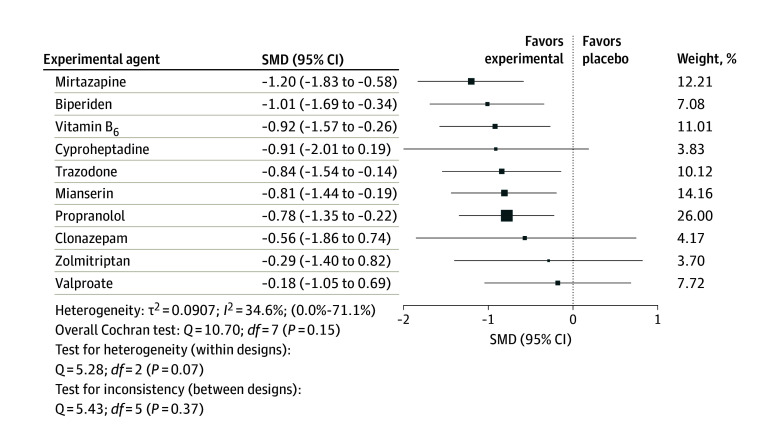
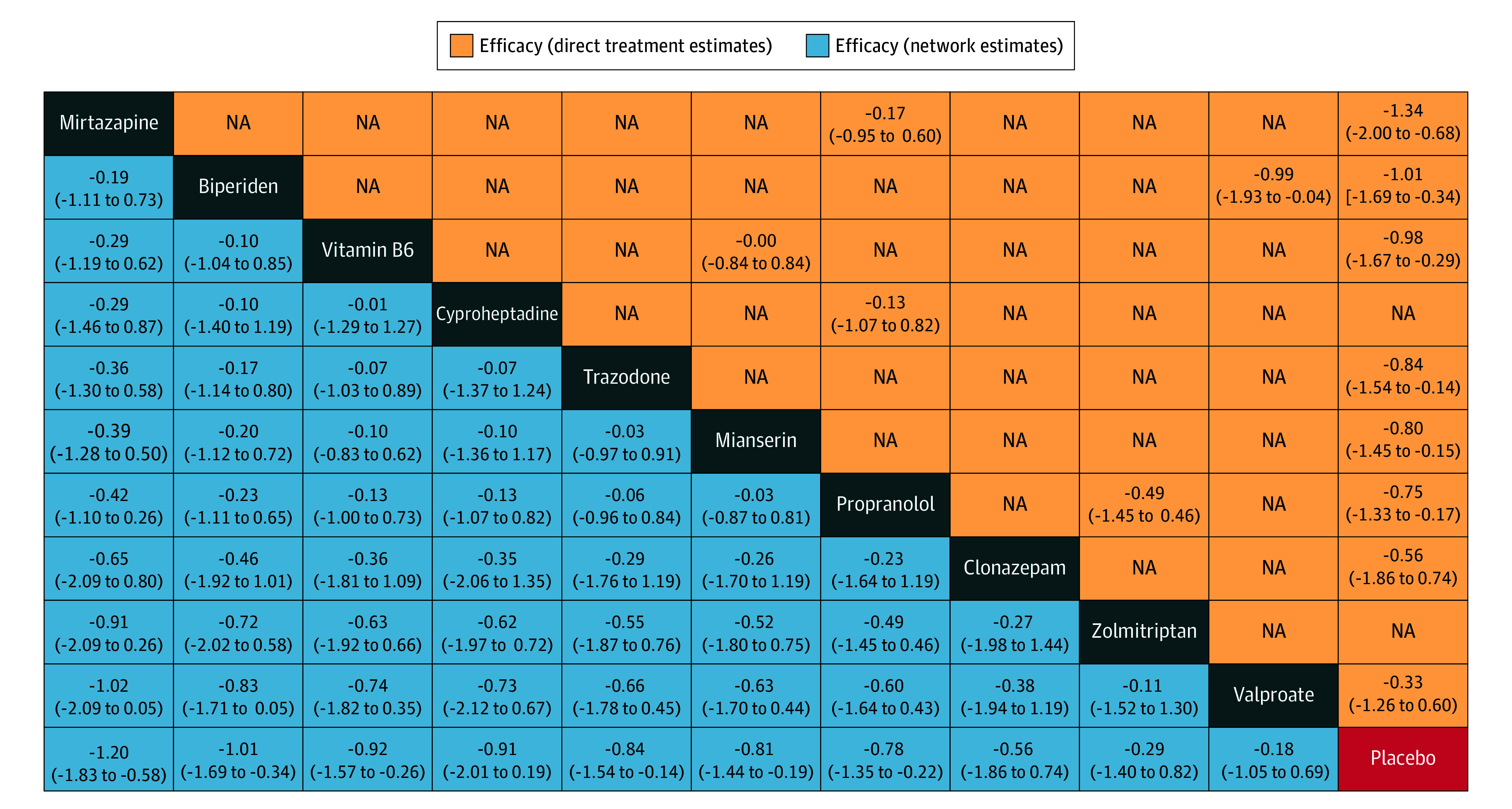
Results: Fifteen trials involving 492 participants compared 10 treatments with placebo. Mirtazapine (15 mg/d for ≥5 days; SMD, -1.20; 95% CI, -1.83 to -0.58), biperiden (6 mg/d for ≥14 days; SMD, -1.01; 95% CI, -1.69 to -0.34), vitamin B6 (600-1200 mg/d for ≥5 days; SMD, -0.92; 95% CI, -1.57 to -0.26), trazodone (50 mg/d for ≥5 days; SMD, -0.84; 95% CI, -1.54 to -0.14), mianserin (15 mg/d for ≥5 days; SMD, -0.81; 95% CI, -1.44 to -0.19), and propranolol (20 mg/d for ≥6 days; SMD, -0.78; 95% CI, -1.35 to -0.22) were associated with greater efficacy than placebo, with low to moderate heterogeneity (I2 = 34.6%; 95% CI, 0.0%-71.1%). Cyproheptadine, clonazepam, zolmitriptan, and valproate did not yield significant effects. Eight trials were rated as having low risk of bias; 2, moderate risk; and 5, high risk. Sensitivity analyses generally confirmed the results for all drugs except for cyproheptadine and propranolol. No association between effect sizes and psychotic severity was found.
Conclusions and relevance: In this systematic review and network meta-analysis, mirtazapine, biperiden, and vitamin B6 were associated with the greatest efficacy for AIA, with vitamin B6 having the best efficacy and tolerance profile. Trazodone, mianserin, and propranolol appeared as effective alternatives with slightly less favorable efficacy and tolerance profiles. These findings should assist prescribers in selecting an appropriate medication for treating AIA.
Conflict of interest statement
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
-
- Huhn M, Nikolakopoulou A, Schneider-Thoma J, et al. . Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394(10202):939-951. doi:10.1016/S0140-6736(19)31135-3 - DOI - PMC - PubMed
