

P2Y12 Inhibitor Monotherapy vs Dual Antiplatelet Therapy After Deployment of a Drug-Eluting Stent: The SHARE Randomized Clinical Trial
- PMID: 38451525
- PMCID: PMC10921250
- DOI: 10.1001/jamanetworkopen.2024.0877
P2Y12 Inhibitor Monotherapy vs Dual Antiplatelet Therapy After Deployment of a Drug-Eluting Stent: The SHARE Randomized Clinical Trial
Erratum in
-
Error in Figure.JAMA Netw Open. 2024 Apr 1;7(4):e2413426. doi: 10.1001/jamanetworkopen.2024.13426. JAMA Netw Open. 2024. PMID: 38656582 Free PMC article. No abstract available.
-
Errors in Figure, Text, and Table.JAMA Netw Open. 2024 Aug 1;7(8):e2434909. doi: 10.1001/jamanetworkopen.2024.34909. JAMA Netw Open. 2024. PMID: 39178004 Free PMC article. No abstract available.
Abstract
Importance: P2Y12 inhibitor monotherapy after dual antiplatelet therapy (DAPT; a P2Y12 inhibitor plus aspirin) for a brief duration has recently emerged as an attractive alternative for patients undergoing percutaneous coronary intervention (PCI) with a drug-eluting stent.
Objective: To investigate whether P2Y12 inhibitor monotherapy after 3 months of DAPT was noninferior to 12 months of DAPT following PCI with a drug-eluting stent.
Design, setting, and participants: The Short-Term Dual Antiplatelet Therapy After Deployment of Bioabsorbable Polymer Everolimus-Eluting Stent (SHARE) open-label, noninferiority randomized clinical trial was conducted from December 15, 2017, through December 14, 2020. Final 1-year clinical follow-up was completed in January 2022. This study was a multicenter trial that was conducted at 20 hospitals in South Korea. Patients who underwent successful PCI with bioabsorbable polymer everolimus-eluting stents were enrolled.
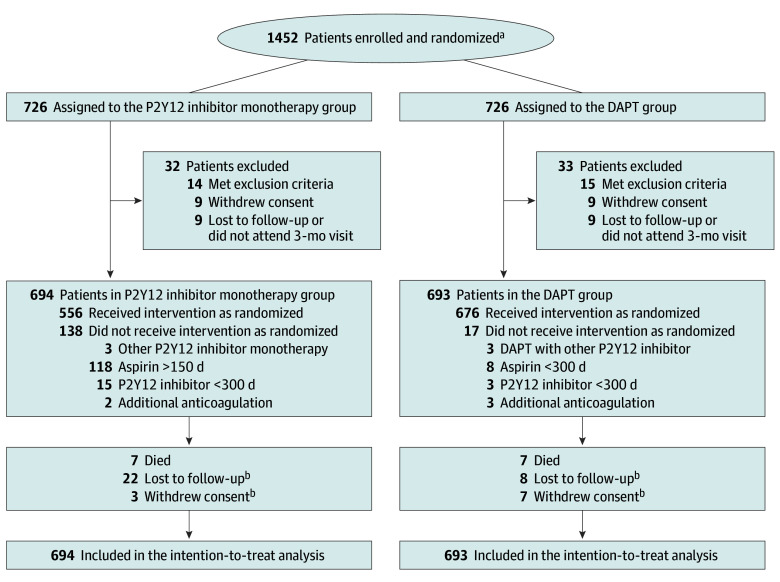
Interventions: Patients were randomly assigned to receive P2Y12 inhibitor monotherapy after 3 months of DAPT (n = 694) or 12 months of DAPT (n = 693).
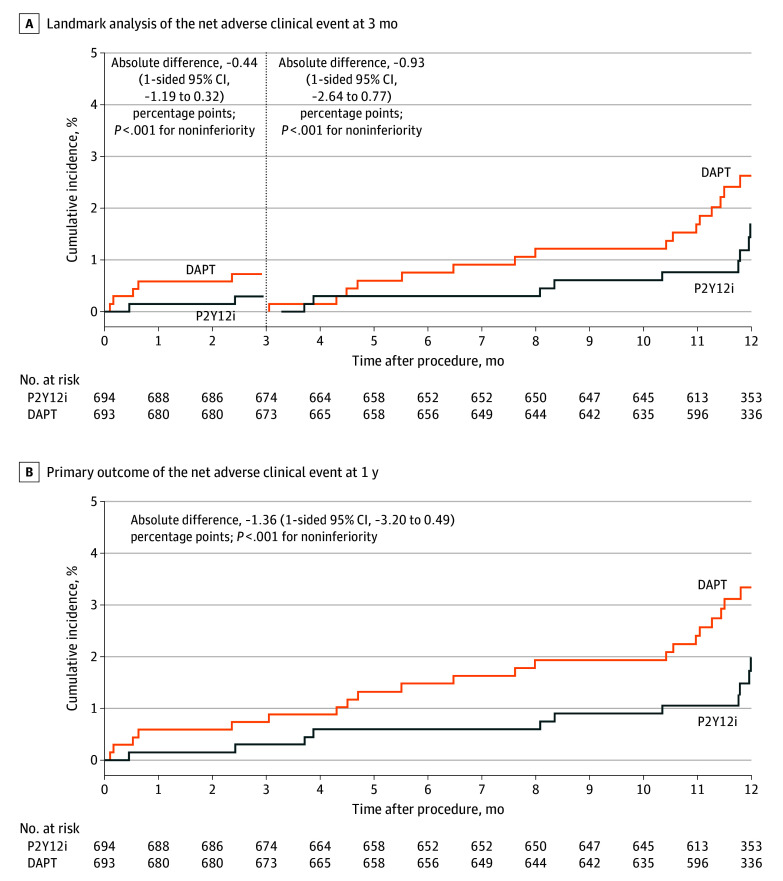
Main outcomes and measures: The primary outcome was a net adverse clinical event, a composite of major bleeding (based on Bleeding Academic Research Consortium type 3 or type 5 bleeding) and major adverse cardiac and cerebrovascular events (cardiac death, myocardial infarction, stent thrombosis, stroke, or ischemia-driven target lesion revascularization) between 3 and 12 months after the index PCI. The major secondary outcomes were major adverse cardiac and cerebrovascular events and major bleeding. The noninferiority margin was 3.0%.
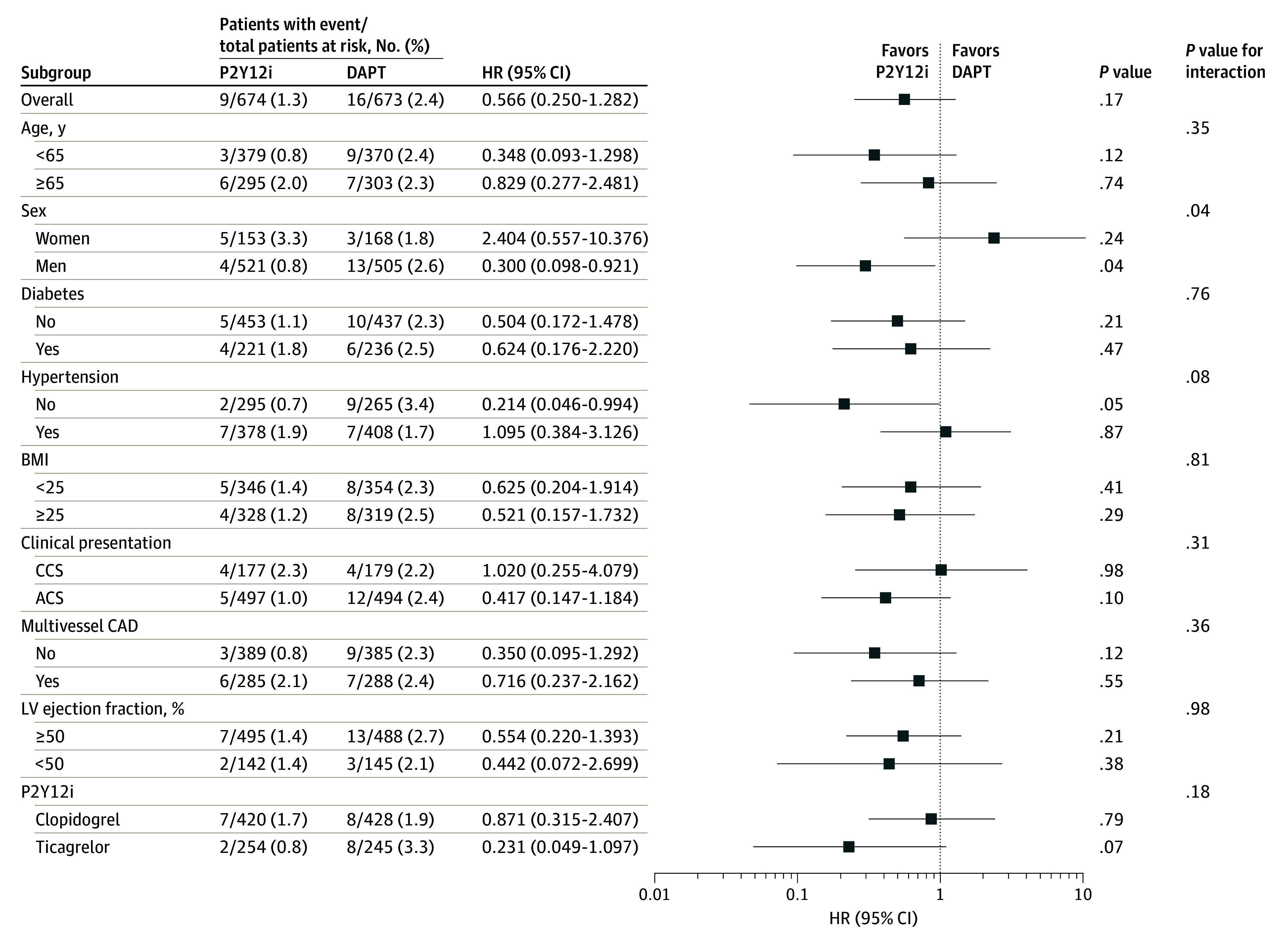
Results: Of the total 1452 eligible patients, 65 patients were excluded before the 3-month follow-up, and 1387 patients (mean [SD] age, 63.0 [10.7] years; 1055 men [76.1%]) were assigned to P2Y12 inhibitor monotherapy (n = 694) or DAPT (n = 693). Between 3 and 12 months of follow-up, the primary outcome (using Kaplan-Meier estimates) occurred in 9 patients (1.7%) in the P2Y12 inhibitor monotherapy group and in 16 patients (2.6%) in the DAPT group (absolute difference, -0.93 [1-sided 95% CI, -2.64 to 0.77] percentage points; P < .001 for noninferiority). For the major secondary outcomes (using Kaplan-Meier estimates), major adverse cardiac and cerebrovascular events occurred in 8 patients (1.5%) in the P2Y12 inhibitor monotherapy group and in 12 patients (2.0%) in the DAPT group (absolute difference, -0.49 [95% CI, -2.07 to 1.09] percentage points; P = .54). Major bleeding occurred in 1 patient (0.2%) in the P2Y12 inhibitor monotherapy group and in 5 patients (0.8%) in the DAPT group (absolute difference, -0.60 [95% CI, -1.33 to 0.12] percentage points; P = .10).
Conclusions and relevance: In patients with coronary artery disease undergoing PCI with the latest generation of drug-eluting stents, P2Y12 inhibitor monotherapy after 3-month DAPT was not inferior to 12-month DAPT for net adverse clinical events. Considering the study population and lower-than-expected event rates, further research is required in other populations.
Trial registration: ClinicalTrials.gov Identifier: NCT03447379.
Conflict of interest statement
Figures
References
-
- Levine GN, Bates ER, Bittl JA, et al. . 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68(10):1082-1115. doi:10.1016/j.jacc.2016.03.513 - DOI - PubMed
-
- Valgimigli M, Bueno H, Byrne RA, et al. ; ESC Scientific Document Group; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies . 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the Task Force for Dual Antiplatelet Therapy in Coronary Artery Disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018;39(3):213-260. doi:10.1093/eurheartj/ehx419 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
