

Deep Learning-based Segmentation of Computed Tomography Scans Predicts Disease Progression and Mortality in Idiopathic Pulmonary Fibrosis
- PMID: 38452227
- PMCID: PMC11351794
- DOI: 10.1164/rccm.202311-2185OC
Deep Learning-based Segmentation of Computed Tomography Scans Predicts Disease Progression and Mortality in Idiopathic Pulmonary Fibrosis
Abstract
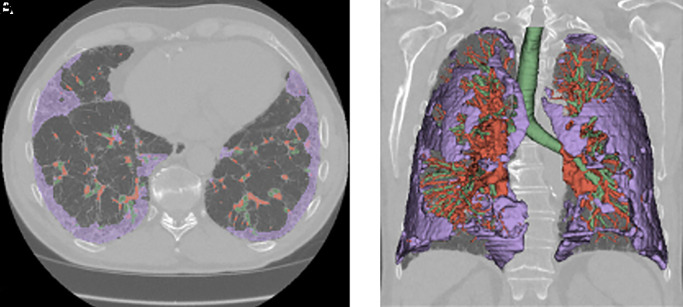
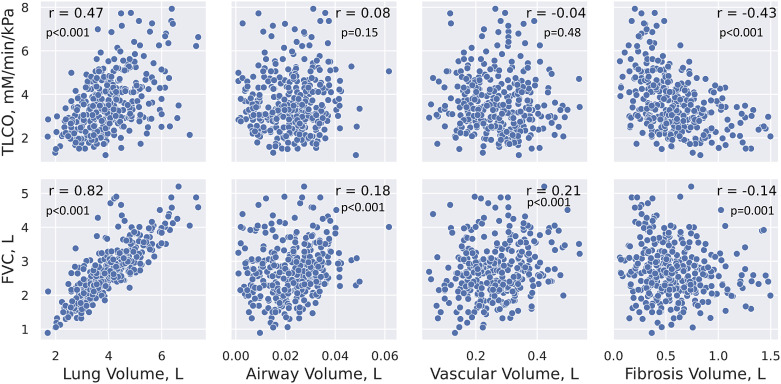
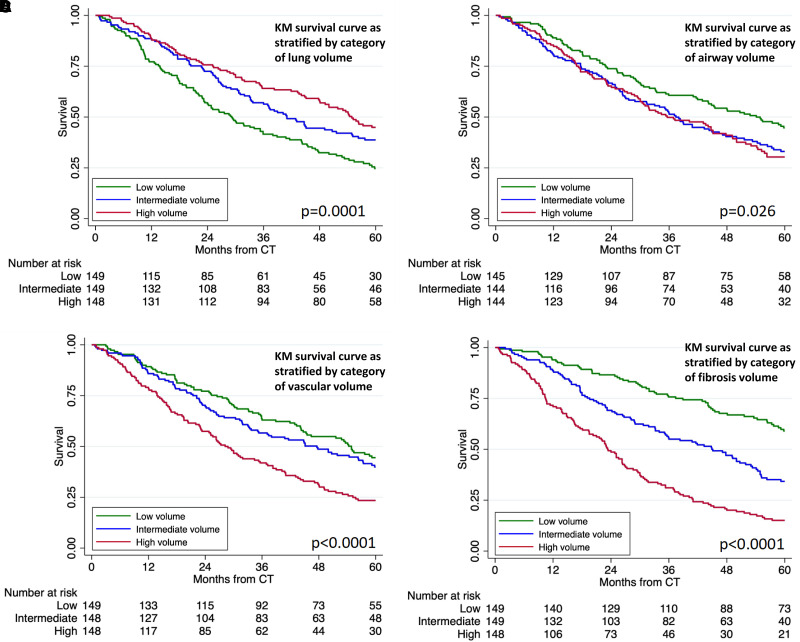
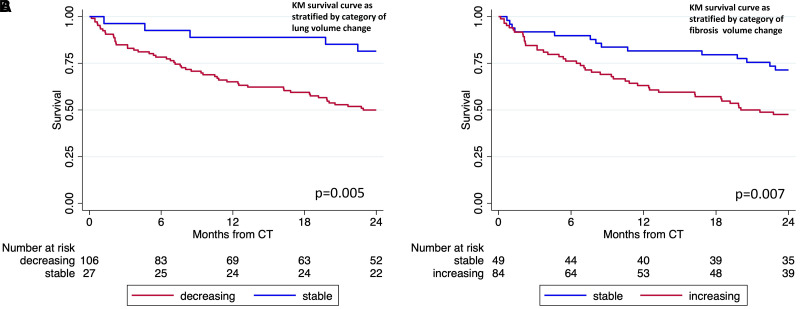
Rationale: Despite evidence demonstrating a prognostic role for computed tomography (CT) scans in idiopathic pulmonary fibrosis (IPF), image-based biomarkers are not routinely used in clinical practice or trials. Objectives: To develop automated imaging biomarkers using deep learning-based segmentation of CT scans. Methods: We developed segmentation processes for four anatomical biomarkers, which were applied to a unique cohort of treatment-naive patients with IPF enrolled in the PROFILE (Prospective Observation of Fibrosis in the Lung Clinical Endpoints) study and tested against a further United Kingdom cohort. The relationships among CT biomarkers, lung function, disease progression, and mortality were assessed. Measurements and Main Results: Data from 446 PROFILE patients were analyzed. Median follow-up duration was 39.1 months (interquartile range, 18.1-66.4 mo), with a cumulative incidence of death of 277 (62.1%) over 5 years. Segmentation was successful on 97.8% of all scans, across multiple imaging vendors, at slice thicknesses of 0.5-5 mm. Of four segmentations, lung volume showed the strongest correlation with FVC (r = 0.82; P < 0.001). Lung, vascular, and fibrosis volumes were consistently associated across cohorts with differential 5-year survival, which persisted after adjustment for baseline gender, age, and physiology score. Lower lung volume (hazard ratio [HR], 0.98 [95% confidence interval (CI), 0.96-0.99]; P = 0.001), increased vascular volume (HR, 1.30 [95% CI, 1.12-1.51]; P = 0.001), and increased fibrosis volume (HR, 1.17 [95% CI, 1.12-1.22]; P < 0.001) were associated with reduced 2-year progression-free survival in the pooled PROFILE cohort. Longitudinally, decreasing lung volume (HR, 3.41 [95% CI, 1.36-8.54]; P = 0.009) and increasing fibrosis volume (HR, 2.23 [95% CI, 1.22-4.08]; P = 0.009) were associated with differential survival. Conclusions: Automated models can rapidly segment IPF CT scans, providing prognostic near and long-term information, which could be used in routine clinical practice or as key trial endpoints.
Keywords: IPF; machine learning.
Figures
Comment in
-
Quantitative Computed Tomography in Idiopathic Pulmonary Fibrosis: Is It Time to Act?Am J Respir Crit Care Med. 2024 Aug 15;210(4):382-383. doi: 10.1164/rccm.202403-0659ED. Am J Respir Crit Care Med. 2024. PMID: 38625082 Free PMC article. No abstract available.
Similar articles
-
Novel Artificial Intelligence-based Technology for Chest Computed Tomography Analysis of Idiopathic Pulmonary Fibrosis.Ann Am Thorac Soc. 2022 Mar;19(3):399-406. doi: 10.1513/AnnalsATS.202101-044OC. Ann Am Thorac Soc. 2022. PMID: 34410886
-
Serial decline in lung volume parameters on computed tomography (CT) predicts outcome in idiopathic pulmonary fibrosis (IPF).Eur Radiol. 2022 Apr;32(4):2650-2660. doi: 10.1007/s00330-021-08338-2. Epub 2021 Oct 30. Eur Radiol. 2022. PMID: 34716781 Free PMC article.
-
Prediction of idiopathic pulmonary fibrosis progression using early quantitative changes on CT imaging for a short term of clinical 18-24-month follow-ups.Eur Radiol. 2020 Feb;30(2):726-734. doi: 10.1007/s00330-019-06402-6. Epub 2019 Aug 26. Eur Radiol. 2020. PMID: 31451973
-
From pixels to prognosis: unlocking the potential of deep learning in fibrotic lung disease imaging analysis.Br J Radiol. 2024 Sep 1;97(1161):1517-1525. doi: 10.1093/bjr/tqae108. Br J Radiol. 2024. PMID: 38781513 Free PMC article. Review.
-
The applications of CT with artificial intelligence in the prognostic model of idiopathic pulmonary fibrosis.Ther Adv Respir Dis. 2024 Jan-Dec;18:17534666241282538. doi: 10.1177/17534666241282538. Ther Adv Respir Dis. 2024. PMID: 39382448 Free PMC article. Review.
Cited by
-
The density histograms-derived computerized integrated index (CII) predicts mortality in idiopathic pulmonary fibrosis.Sci Rep. 2024 Dec 28;14(1):30680. doi: 10.1038/s41598-024-77328-3. Sci Rep. 2024. PMID: 39730381 Free PMC article.
-
Advances in idiopathic pulmonary fibrosis diagnosis and treatment.Chin Med J Pulm Crit Care Med. 2025 Mar 7;3(1):12-21. doi: 10.1016/j.pccm.2025.02.001. eCollection 2025 Mar. Chin Med J Pulm Crit Care Med. 2025. PMID: 40226606 Free PMC article. Review.
-
Radiomics and Artificial Intelligence in Pulmonary Fibrosis.J Imaging Inform Med. 2025 Jan 6. doi: 10.1007/s10278-024-01377-3. Online ahead of print. J Imaging Inform Med. 2025. PMID: 39762544 Review.
-
A systematic review of the role of quantitative CT in the prognostication and disease monitoring of interstitial lung disease.Eur Respir Rev. 2025 Apr 30;34(176):240194. doi: 10.1183/16000617.0194-2024. Print 2025 Apr. Eur Respir Rev. 2025. PMID: 40306954 Free PMC article.
-
Radiomics-Based Artificial Intelligence and Machine Learning Approach for the Diagnosis and Prognosis of Idiopathic Pulmonary Fibrosis: A Systematic Review.Cureus. 2025 Jul 7;17(7):e87461. doi: 10.7759/cureus.87461. eCollection 2025 Jul. Cureus. 2025. PMID: 40772136 Free PMC article. Review.
References
-
- Karimi-Shah BA, Chowdhury BA. Forced vital capacity in idiopathic pulmonary fibrosis—FDA review of pirfenidone and nintedanib. N Engl J Med . 2015;372:1189–1191. - PubMed
-
- Israël-Biet D, Juvin K, Dang Tran K, Badia A, Cazes A, Delclaux C. Idiopathic pulmonary fibrosis: diagnosis and treatment in 2013 [in French] Rev Pneumol Clin . 2014;70:108–117. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
