

Prognostic value of histopathologic traits independent of stromal tumor-infiltrating lymphocyte levels in chemotherapy-naïve patients with triple-negative breast cancer
- PMID: 38452438
- PMCID: PMC10937239
- DOI: 10.1016/j.esmoop.2024.102923
Prognostic value of histopathologic traits independent of stromal tumor-infiltrating lymphocyte levels in chemotherapy-naïve patients with triple-negative breast cancer
Abstract
Background: In the absence of prognostic biomarkers, most patients with early-stage triple-negative breast cancer (eTNBC) are treated with combination chemotherapy. The identification of biomarkers to select patients for whom treatment de-escalation or escalation could be considered remains an unmet need. We evaluated the prognostic value of histopathologic traits in a unique cohort of young, (neo)adjuvant chemotherapy-naïve patients with early-stage (stage I or II), node-negative TNBC and long-term follow-up, in relation to stromal tumor-infiltrating lymphocytes (sTILs) for which the prognostic value was recently reported.
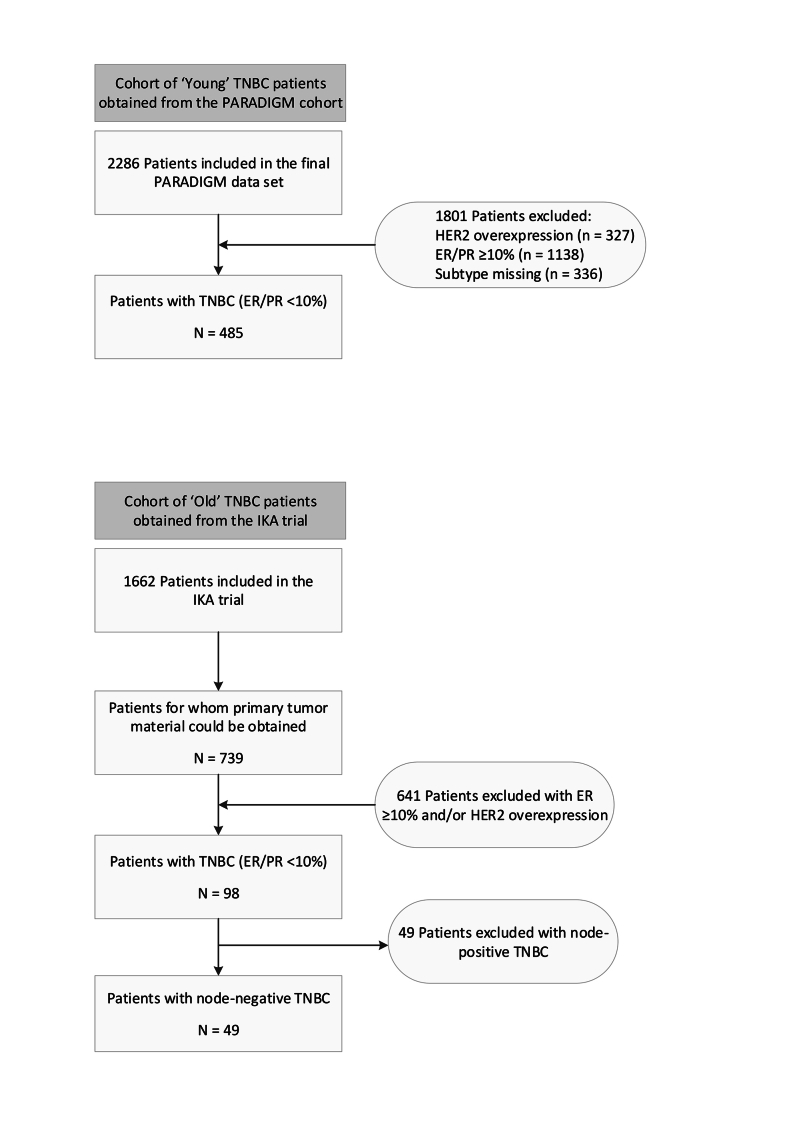
Materials and methods: We studied all 485 patients with node-negative eTNBC from the population-based PARADIGM cohort which selected women aged <40 years diagnosed between 1989 and 2000. None of the patients had received (neo)adjuvant chemotherapy according to standard practice at the time. Associations between histopathologic traits and breast cancer-specific survival (BCSS) were analyzed with Cox proportional hazard models.
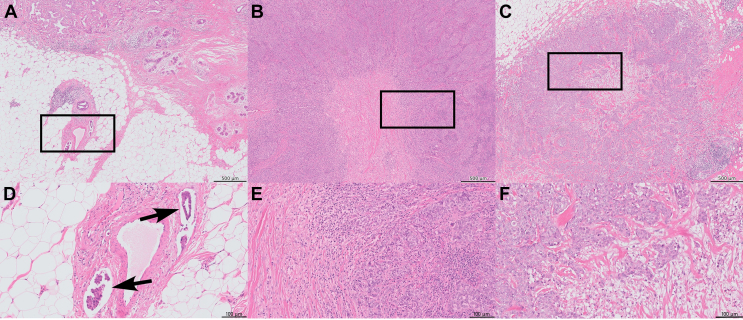
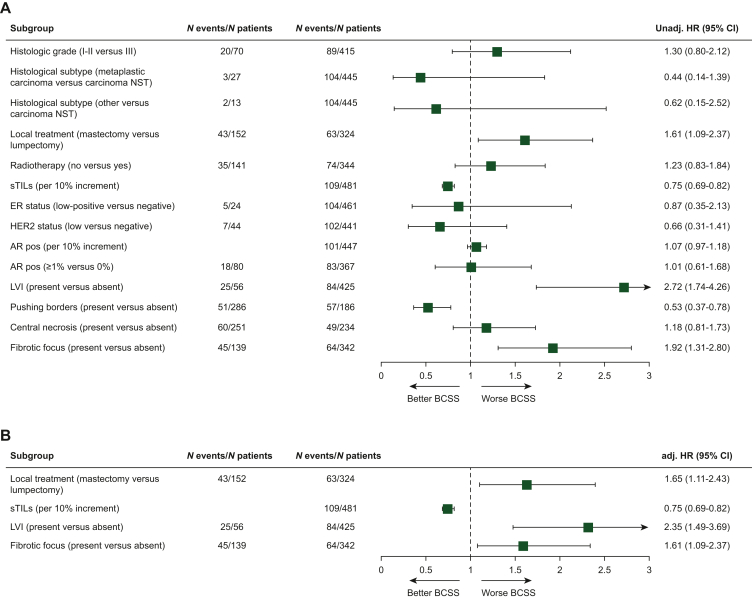
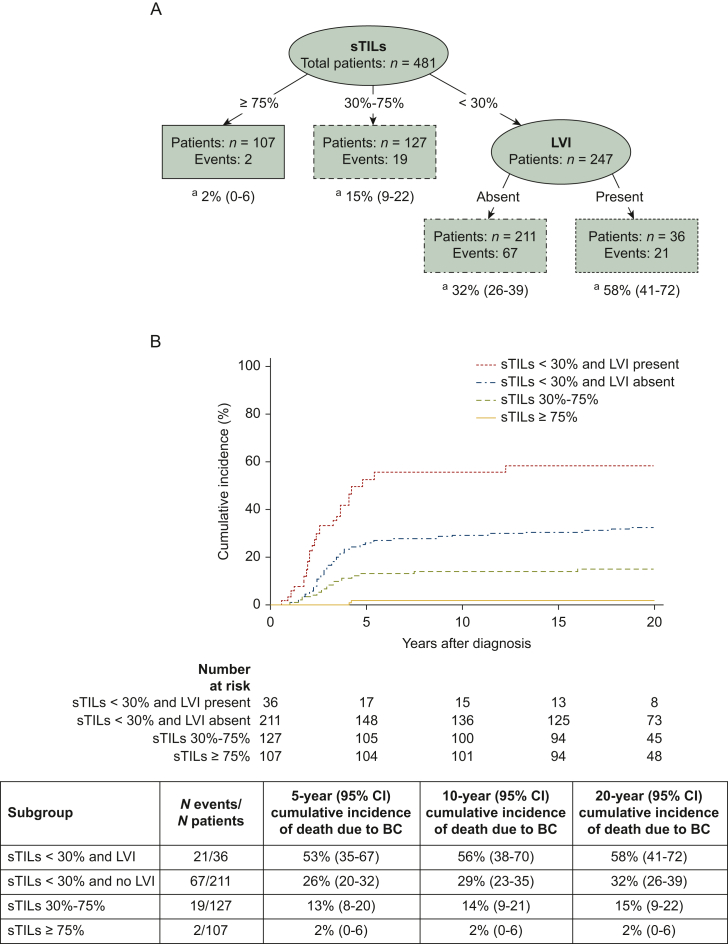
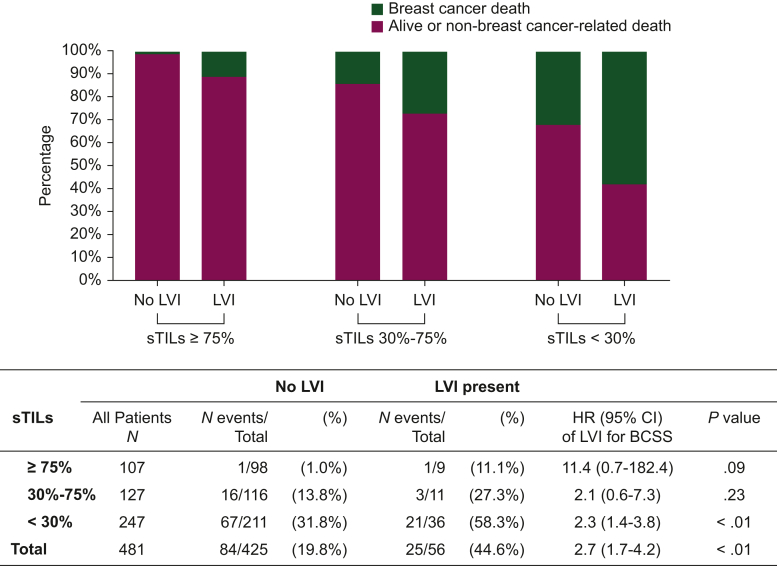
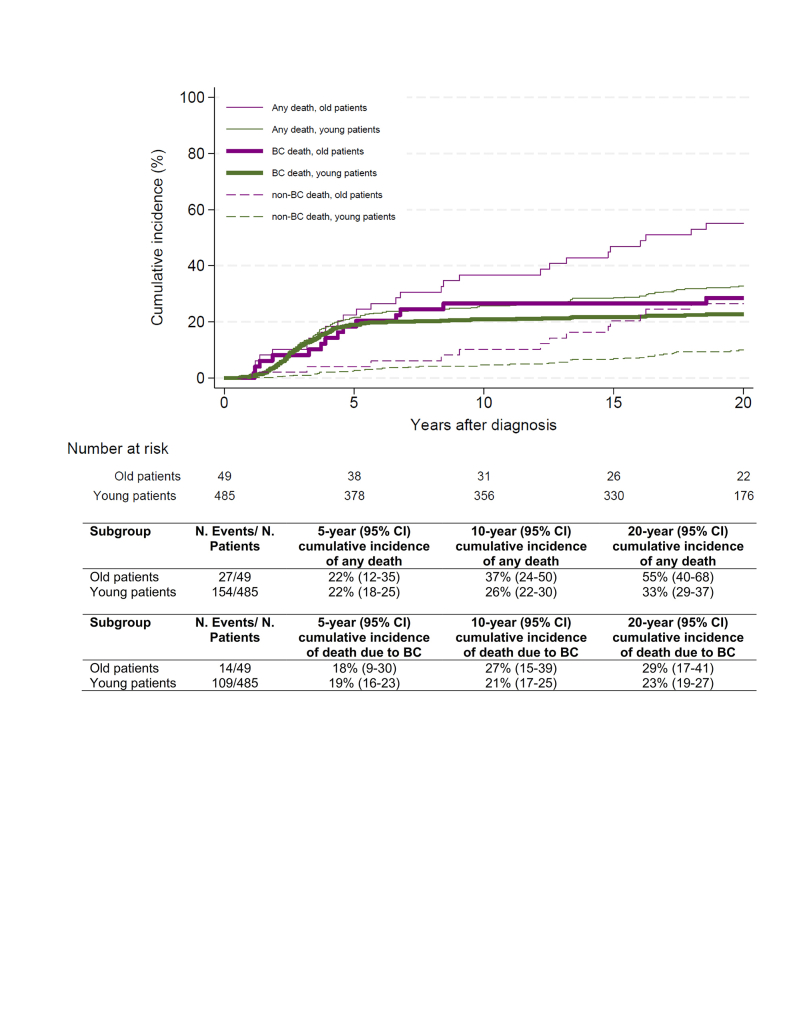
Results: With a median follow-up of 20.0 years, an independent prognostic value for BCSS was observed for lymphovascular invasion (LVI) [adjusted (adj.) hazard ratio (HR) 2.35, 95% confidence interval (CI) 1.49-3.69], fibrotic focus (adj. HR 1.61, 95% CI 1.09-2.37) and sTILs (per 10% increment adj. HR 0.75, 95% CI 0.69-0.82). In the sTILs <30% subgroup, the presence of LVI resulted in a higher cumulative incidence of breast cancer death (at 20 years, 58%; 95% CI 41% to 72%) compared with when LVI was absent (at 20 years, 32%; 95% CI 26% to 39%). In the ≥75% sTILs subgroup, the presence of LVI might be associated with poor survival (HR 11.45, 95% CI 0.71-182.36, two deaths). We confirm the lack of prognostic value of androgen receptor expression and human epidermal growth factor receptor 2 -low status.
Conclusions: sTILs, LVI and fibrotic focus provide independent prognostic information in young women with node-negative eTNBC. Our results are of importance for the selection of patients for de-escalation and escalation trials.
Keywords: fibrotic focus; lymphovascular invasion; prognostic biomarkers; stromal tumor-infiltrating lymphocytes; triple-negative breast cancer.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure PJvD has advisory relationships with Paige, Pantarei and Samantree, paid to the institution, and research grants paid to the institute from Pfizer. NS received institutional research funding from Pfizer. ZV has a consulting role for Roche. CHMvD received institutional research funding from AstraZeneca/Daiichi Sankyo. SMW has a consulting role for Roche, and received institutional research funding from Roche, Pfizer, Bayer, MSD, AstraZeneca/Merck and Amgen. SMW has a consulting role for IDDI, Sensorion, Biophytis, Servier, Yuhan, Amaris Consulting and Roche. JW received institutional research funding from Cancer Research UK and KWF Dutch Cancer Society. AR has a consulting role for MSD Oncology, Amgen, Roche, AstraZeneca/Daiichi Sankyo and Bristol Myers Squibb/Pfizer. SCL reports grants from ZonMw and A Sister’s Hope during the conduct of the study; has been an advisory board member for AstraZeneca, Cergentis, IBM, Novartis, Pfizer, Sanofi and Roche; and received institutional research grants from Agendia, AstraZeneca, Eurocept-pharmaceuticals and Merck and Pfizer. In addition, SCL received institutional research grants and institutional non-financial support from Agendia, Genentech, Novartis, Roche, Tesaro and Immunomedics and other institutional support from AstraZeneca, Pfizer, Cergentis, Daiichi Sankyo, IBM and Bayer outside the submitted work. MK is an advisory board member and/or received speakers’ fee for/from Alderaan, Bristol Myers Squibb (BMS), Domain Therapeutics, Gilead, Roche, Medscape, MSD and AZ/Daiichi and received institutional research support from AstraZeneca/Daiichi, BMS and Roche outside the submitted work. RS reports non-financial support from Merck and BMS, research support from Merck, Puma Biotechnology and Roche, and personal fees from Roche, BMS and Exact Sciences for advisory boards. IRK received research grants from Novartis and Gilead. RHTK is an advisory board member for Amgen, AstraZeneca, Bayer, BMS, MSD, Novartis, Pfizer, Pierre Fabre Sante, Sanofi and Servier. All other authors have declared no conflicts of interest.
Figures
References
-
- Partridge A.H., Hughes M.E., Warner E.T., et al. Subtype-dependent relationship between young age at diagnosis and breast cancer survival. J Clin Oncol. 2016;34(27):3308–3314. - PubMed
-
- Dent R., Trudeau M., Pritchard K.I., et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13(15 Pt 1):4429–4434. - PubMed
-
- Cardoso F., Kyriakides S., Ohno S., et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(8):1194–1220. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
