

Effectiveness of shared medical appointments delivered in primary care for improving health outcomes in patients with long-term conditions: a systematic review of randomised controlled trials
- PMID: 38453205
- PMCID: PMC10921542
- DOI: 10.1136/bmjopen-2022-067252
Effectiveness of shared medical appointments delivered in primary care for improving health outcomes in patients with long-term conditions: a systematic review of randomised controlled trials
Abstract
Objectives: To examine the effectiveness of shared medical appointments (SMAs) compared with one-to-one appointments in primary care for improving health outcomes and reducing demand on healthcare services by people with one or more long-term conditions (LTCs).
Design: A systematic review of the published literature.
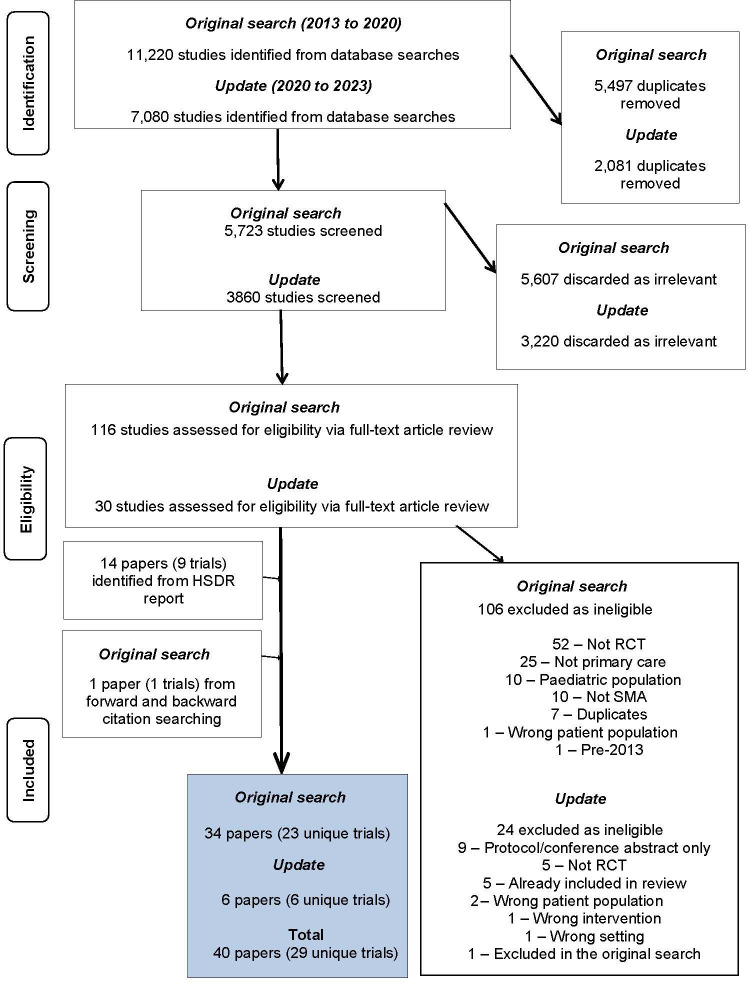
Data sources: Six databases, including MEDLINE and Web of Science, were searched 2013-2023. Relevant pre-2013 trials identified by forward and backward citation searches of the included trials were included.
Eligibility criteria: Randomised controlled trials of SMAs delivered in a primary care setting involving adults over 18 years with one or more LTCs. Studies were excluded if the SMA did not include one-to-one patient-clinician time. All countries were eligible for inclusion.
Data extraction and synthesis: Data were extracted and outcomes narratively synthesised, meta-analysis was undertaken where possible.
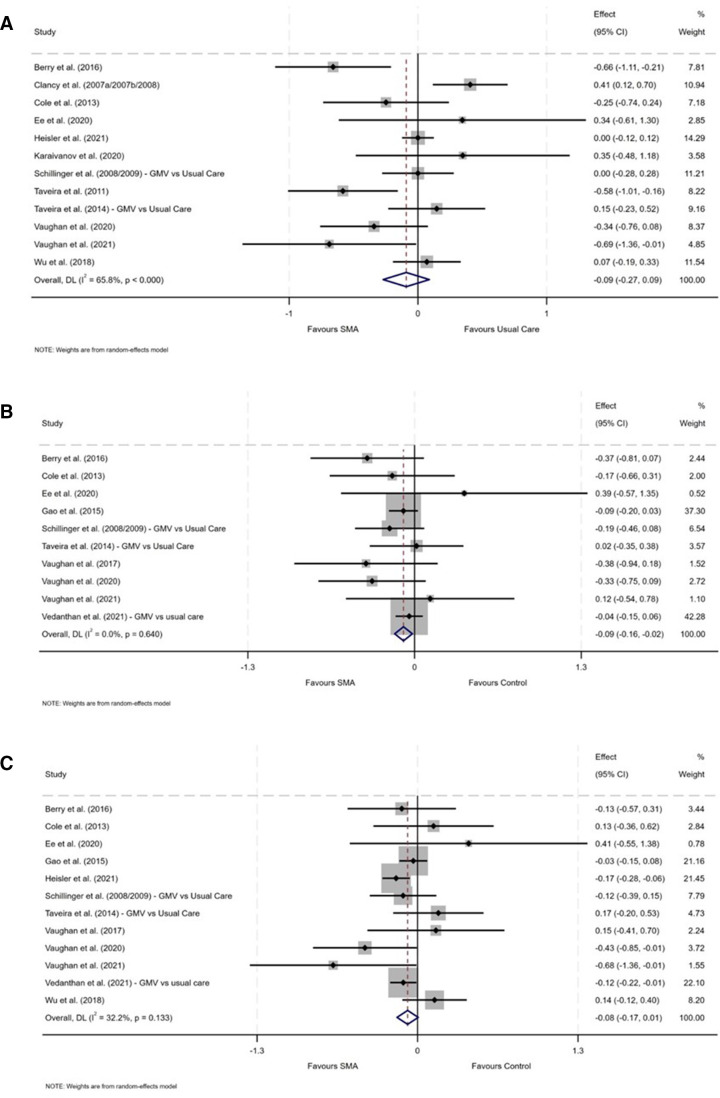
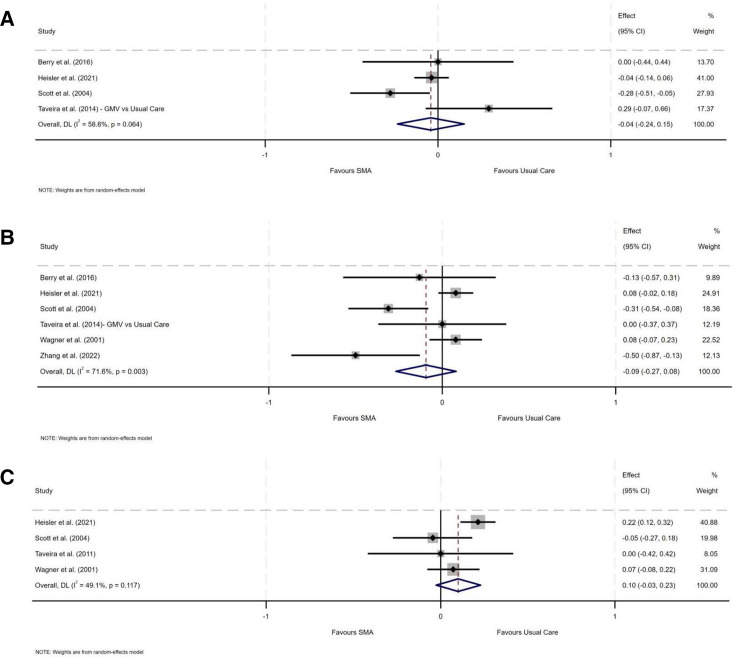
Results: Twenty-nine unique trials were included. SMA models varied in terms of components, mode of delivery and target population. Most trials recruited patients with a single LTC, most commonly diabetes (n=16). There was substantial heterogeneity in outcome measures. Meta-analysis showed that participants in SMA groups had lower diastolic blood pressure than those in usual care (d=-0.086, 95% CI=-0.16 to -0.02, n=10) (p=0.014). No statistically significant differences were found across other outcomes. Compared with usual care, SMAs had no significant effect on healthcare service use. For example, no difference between SMAs and usual care was found for admissions to emergency departments at follow-up (d=-0.094, 95% CI=-0.27 to 0.08, n=6, p=0.289).
Conclusions: There was a little difference in the effectiveness of SMAs compared with usual care in terms of health outcomes or healthcare service use in the short-term (range 12 weeks to 24 months). To strengthen the evidence base, future studies should include a wider array of LTCs, standardised outcome measures and more details on SMA components to help inform economic evaluation.
Prospero registration number: CRD42020173084.
Keywords: Health policy; Organisation of health services; PRIMARY CARE.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Clay H, Stern R. Making time in general practice: freeing GP capacity by reducing bureaucracy and avoidable consultations, managing the interface with hospitals and exploring new ways of working. 2015. Available: https://thehealthcreationalliance.org/wp-content/uploads/2018/11/Making-...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources