

Clinical Evaluation of a 2-Minute Ultrafast Brain MR Protocol for Evaluation of Acute Pathology in the Emergency and Inpatient Settings
- PMID: 38453413
- PMCID: PMC11288578
- DOI: 10.3174/ajnr.A8143
Clinical Evaluation of a 2-Minute Ultrafast Brain MR Protocol for Evaluation of Acute Pathology in the Emergency and Inpatient Settings
Abstract
Background and purpose: The use of MR imaging in emergency settings has been limited by availability, long scan times, and sensitivity to motion. This study assessed the diagnostic performance of an ultrafast brain MR imaging protocol for evaluation of acute intracranial pathology in the emergency department and inpatient settings.
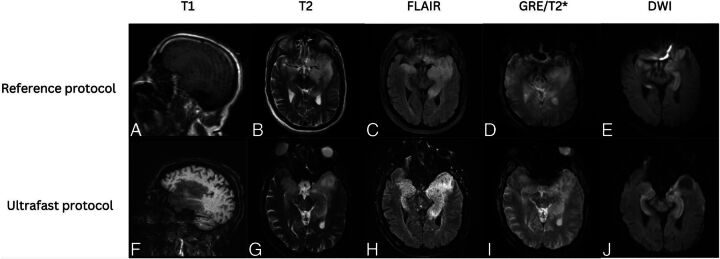
Materials and methods: Sixty-six adult patients who underwent brain MR imaging in the emergency department and inpatient settings were included in the study. All patients underwent both the reference and the ultrafast brain MR protocols. Both brain MR imaging protocols consisted of T1-weighted, T2/T2*-weighted, FLAIR, and DWI sequences. The ultrafast MR images were reconstructed by using a machine-learning assisted framework. All images were reviewed by 2 blinded neuroradiologists.
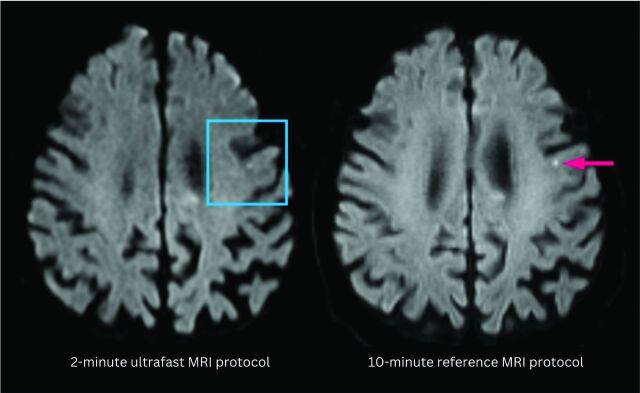
Results: The average acquisition time was 2.1 minutes for the ultrafast brain MR protocol and 10 minutes for the reference brain MR protocol. There was 98.5% agreement on the main clinical diagnosis between the 2 protocols. In head-to-head comparison, the reference protocol was preferred in terms of image noise and geometric distortion (P < .05 for both). The ultrafast ms-EPI protocol was preferred over the reference protocol in terms of reduced motion artifacts (P < .01). Overall diagnostic quality was not significantly different between the 2 protocols (P > .05).
Conclusions: The ultrafast brain MR imaging protocol provides high accuracy for evaluating acute pathology while only requiring a fraction of the scan time. Although there was greater image noise and geometric distortion on the ultrafast brain MR protocol images, there was significant reduction in motion artifacts with similar overall diagnostic quality between the 2 protocols.
© 2024 by American Journal of Neuroradiology.
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical