

S100A9+CD14+ monocytes contribute to anti-PD-1 immunotherapy resistance in advanced hepatocellular carcinoma by attenuating T cell-mediated antitumor function
- PMID: 38454445
- PMCID: PMC10921725
- DOI: 10.1186/s13046-024-02985-1
S100A9+CD14+ monocytes contribute to anti-PD-1 immunotherapy resistance in advanced hepatocellular carcinoma by attenuating T cell-mediated antitumor function
Abstract
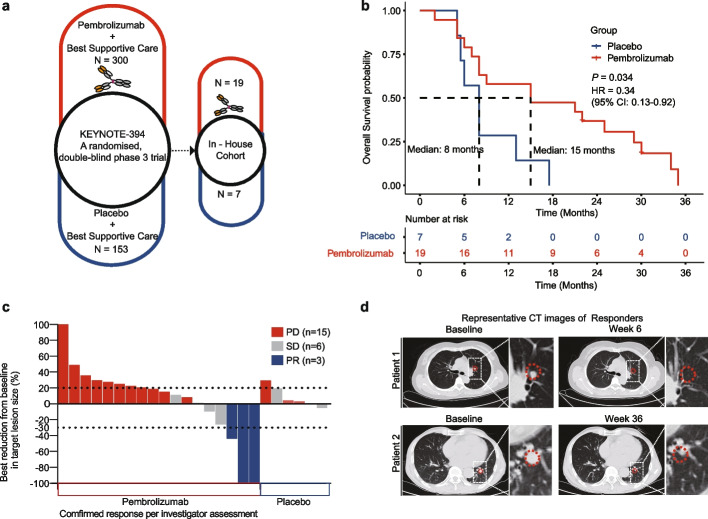
Background: The paucity of reliable biomarkers for predicting immunotherapy efficacy in patients with advanced hepatocellular carcinoma (HCC) has emerged as a burgeoning concern with the expanding use of immunotherapy. This study endeavors to delve into the potential peripheral biomarkers capable of prognosticating efficacy in HCC patients who are poised to receive anti-PD-1 monotherapy within the phase III clinical trial, KEYNOTE394. Additionally, we sought to elucidate the underlying molecular mechanisms for resistance to immune checkpoint blockade (ICB) and propose innovative combination immunotherapy strategies for future clinical application.
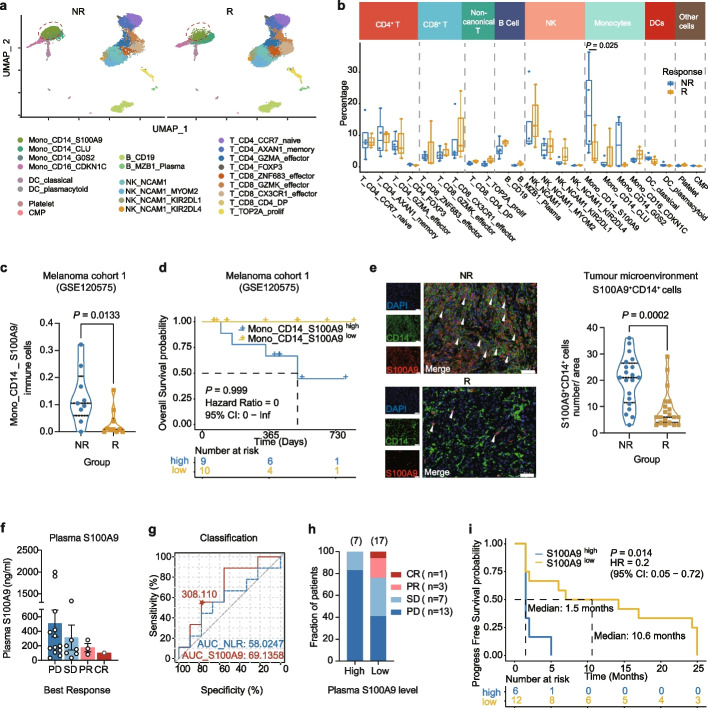
Methods: Patient blood samples were collected for single-cell RNA sequencing to evaluate the immune cell signature before receiving ICB therapy. Subsequently, in vitro assays and in vivo murine model experiments were conducted to validate the mechanism that S100A9+CD14+ monocytes play a role in ICB resistance.
Results: Our study demonstrates a notable enrichment of S100A9+CD14+ monocytes in the peripheral blood of patients exhibiting suboptimal responses to anti-PD-1 therapy. Moreover, we identified the Mono_S100A9 signature as a predictive biomarker, indicative of reduced efficacy in immunotherapy and decreased survival benefits across various tumor types. Mechanistically, S100A9 activates PD-L1 transcription by directly binding to the CD274 (PD-L1) gene promoter, thereby suppressing T-cell proliferation and cytotoxicity via the PD-1/PD-L1 axis, consequently diminishing the therapeutic effectiveness of subsequent anti-PD-1 treatments. Furthermore, our in vivo studies revealed that inhibiting S100A9 can synergistically enhance the efficacy of anti-PD-1 drugs in the eradication of hepatocellular carcinoma.
Conclusions: Our study underscores the significance of S100A9+CD14+ monocytes in predicting inadequate response to ICB treatment and provides insights into the monocyte cell-intrinsic mechanisms of resistance to ICB therapy. We also propose a combined therapeutic approach to enhance ICB efficacy by targeting S100A9.
Keywords: Anti-PD-1 monotherapy; Biomarker; Hepatocellular carcinoma; S100A9+CD14+ monocyte; Single-cell RNA sequencing.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interests.
Figures






References
-
- El-Khoueiry AB, Sangro B, Yau T, Crocenzi TS, Kudo M, Hsu C, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet (London, England) 2017;389(10088):2492–2502. doi: 10.1016/S0140-6736(17)31046-2. - DOI - PMC - PubMed
-
- Zhu AX, Finn RS, Edeline J, Cattan S, Ogasawara S, Palmer D, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi: 10.1016/S1470-2045(18)30351-6. - DOI - PubMed
-
- Xu J, Shen J, Gu S, Zhang Y, Wu L, Wu J, et al. Camrelizumab in Combination with Apatinib in Patients with Advanced Hepatocellular Carcinoma (RESCUE): A Nonrandomized, Open-label. Phase II Trial Clin Cancer Res. 2021;27(4):1003–1011. - PubMed
MeSH terms
Substances
Grants and funding
- Z24C080003/Natural Science Foundation of Zhejiang Province
- LD21C070001/Natural Science Foundation of Zhejiang Province
- U21A20356/National Natural Science Foundation of China
- 82202875/National Natural Science Foundation of China
- 02020200-K02013007/ZJU-Hangzhou Global Scientific and Technological Innovation Center, Zhejiang University
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
