

Pathophysiology of acute lung injury in patients with acute brain injury: the triple-hit hypothesis
- PMID: 38454447
- PMCID: PMC10918982
- DOI: 10.1186/s13054-024-04855-w
Pathophysiology of acute lung injury in patients with acute brain injury: the triple-hit hypothesis
Abstract
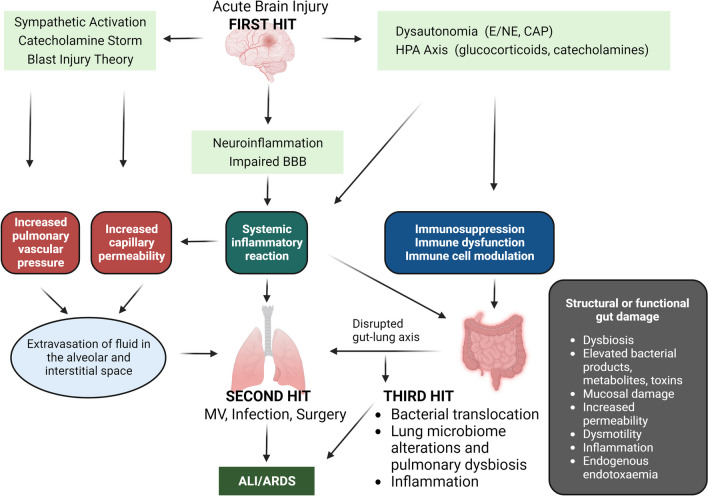
It has been convincingly demonstrated in recent years that isolated acute brain injury (ABI) may cause severe dysfunction of peripheral extracranial organs and systems. Of all potential target organs and systems, the lung appears to be the most vulnerable to damage after ABI. The pathophysiology of the bidirectional brain-lung interactions is multifactorial and involves inflammatory cascades, immune suppression, and dysfunction of the autonomic system. Indeed, the systemic effects of inflammatory mediators in patients with ABI create a systemic inflammatory environment ("first hit") that makes extracranial organs vulnerable to secondary procedures that enhance inflammation, such as mechanical ventilation (MV), surgery, and infections ("second hit"). Moreover, accumulating evidence supports the knowledge that gut microbiota constitutes a critical superorganism and an organ on its own, potentially modifying various physiological functions of the host. Furthermore, experimental and clinical data suggest the existence of a communication network among the brain, gastrointestinal tract, and its microbiome, which appears to regulate immune responses, gastrointestinal function, brain function, behavior, and stress responses, also named the "gut-microbiome-brain axis." Additionally, recent research evidence has highlighted a crucial interplay between the intestinal microbiota and the lungs, referred to as the "gut-lung axis," in which alterations during critical illness could result in bacterial translocation, sustained inflammation, lung injury, and pulmonary fibrosis. In the present work, we aimed to further elucidate the pathophysiology of acute lung injury (ALI) in patients with ABI by attempting to develop the "double-hit" theory, proposing the "triple-hit" hypothesis, focused on the influence of the gut-lung axis on the lung. Particularly, we propose, in addition to sympathetic hyperactivity, blast theory, and double-hit theory, that dysbiosis and intestinal dysfunction in the context of ABI alter the gut-lung axis, resulting in the development or further aggravation of existing ALI, which constitutes the "third hit."
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
