

Exploring the potential of fully automated LUMIPULSE G plasma assays for detecting Alzheimer's disease pathology
- PMID: 38454502
- PMCID: PMC10918996
- DOI: 10.1186/s13195-024-01397-9
Exploring the potential of fully automated LUMIPULSE G plasma assays for detecting Alzheimer's disease pathology
Abstract
Background: LUMIPULSE G-automated immunoassays represent a widely used method for the quantification of Alzheimer's disease (AD) biomarkers in the cerebrospinal fluid (CSF). Less invasive blood-based markers confer a promising tool for AD diagnosis at prodromal stages (mild cognitive impairment (MCI)). Highly sensitive assays for the quantification of amyloid-beta (Aβ) and phosphorylated Tau-181 (p-Tau181) in the blood are showing promising results. In this study, we evaluated the clinical performance of the recently available fully automated LUMIPULSE plasma marker assays for detecting brain AD pathology and for predicting progression from MCI to AD dementia stage.
Methods: A retrospective exploratory cohort of 138 individuals (22 neurological controls [NC], 72 MCI, and 44 AD dementia patients) was included. Data regarding baseline CSF concentrations of Aβ42, Aβ40, t-Tau, and p-Tau181 was available and used to establish the presence of AD brain pathology. Baseline Aβ42, Aβ40, and p-Tau181 concentrations were determined in stored plasma samples using high-throughput fully automated LUMIPULSE assays. Progression from MCI to AD dementia was evaluated during follow-up (mean 6.4 ± 2.5 years). Moreover, a prospective validation cohort of 72 individuals with memory complaints underwent AD biomarker quantification, closely mirroring typical clinical practice. This cohort aimed to confirm the study's main findings.
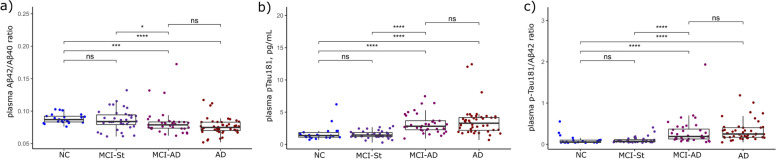
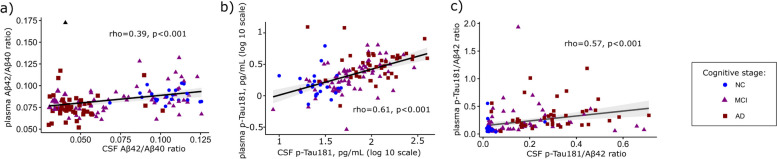
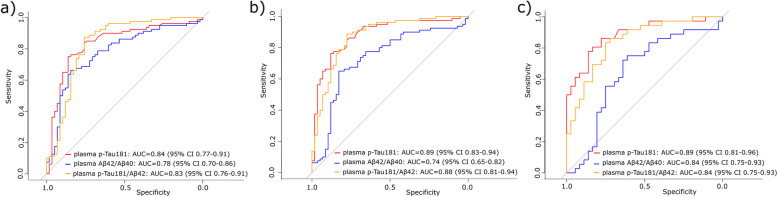
Results: In the exploratory cohort, correlations between CSF and plasma were moderate for p-Tau181 (ρ = 0.61, p < 0.001) and weak for Aβ42/Aβ40 ratio (ρ = 0.39, p < 0.001). Plasma p-Tau181 and p-Tau181/Aβ42 concentrations were significantly increased while Aβ42/Aβ40 was significantly decreased (p < 0.001) in patients with AD dementia and prodromal AD, as well as in individuals with CSF abnormal amyloid concentrations (A +). Plasma p-Tau181 showed a robust performance in differentiating patients clinically diagnosed as AD (AUC = 0.89; 95% CI 0.83-0.94); A + vs. A - (AUC = 0.84, 95% CI 0.77-0.91) and also in predicting conversion to AD dementia in MCI patients (AUC = 0.89, 95% CI 0.81-0.96). When tested in the validation cohort, plasma p-Tau181 displayed 83.3% of the overall percentage of agreement according to amyloid status.
Conclusions: Our results show that the measurement of p-Tau181 in plasma has great potential as a non-invasive prognostic screening tool for implementation in a clinical setting.
Keywords: Alzheimer’s disease; Automated; Early detection; Plasma biomarkers.
© 2024. The Author(s).
Conflict of interest statement
A.N. and N.LB. are employees of Fujirebio S.L. and N.V., respectively.
Figures
References
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A, Holtzmn DM, Jaqust WJ, Petersen RC, Synder PJ, Carrillo MC, Thies B, Phelps CH. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:270–279. doi: 10.1016/j.jalz.2011.03.008. - DOI - PMC - PubMed
-
- Jack CR, Jr, Bennett DA, Blennow K, Carrillo MC, Dunn B, Haeberlein SB, Holtzman DM, Jagust W, Jessen F, Karlawish J, Liu E, Molinuevo JL, Montine T, Phelps C, Rankin KP, Rowe CC, Scheltens P, Siemers E, Snyder HM, Sperling R, Contributors NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018;14(4):535–562. doi: 10.1016/j.jalz.2018.02.018. - DOI - PMC - PubMed
-
- Jack CR, Jr, Knopman DS, Jagust WJ, Petersen RC, Weiner MW, Aisen PS, Shaw LM, Vemuri P, Wiste HJ, Weigand SD, Lesnick TG, Pankratz VS, Donohue MC, Trojanowski JQ. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013;12(2):207–216. doi: 10.1016/S1474-4422(12)70291-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
