

Indocyanine green-enhanced transpupillary thermotherapy for juxtapapillary retinal capillary hemangioblastoma
- PMID: 38454849
- PMCID: PMC11451779
- DOI: 10.4103/IJO.IJO_1684_23
Indocyanine green-enhanced transpupillary thermotherapy for juxtapapillary retinal capillary hemangioblastoma
Abstract
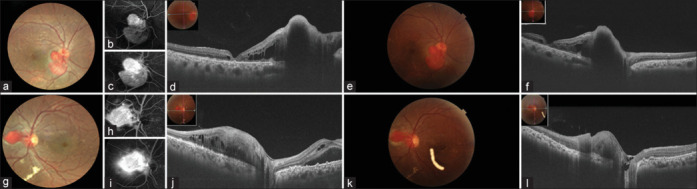
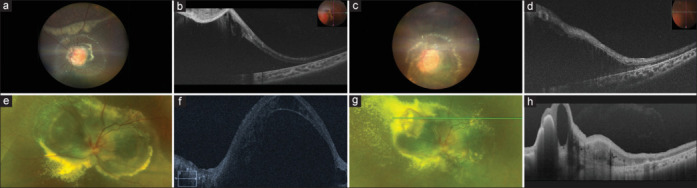
Purpose: To study the clinical presentation and treatment outcomes of indocyanine green-enhanced transpupillary thermotherapy (ICG-TTT) for treatment-naïve juxtapapillary retinal capillary hemangioblastoma (JRCH).
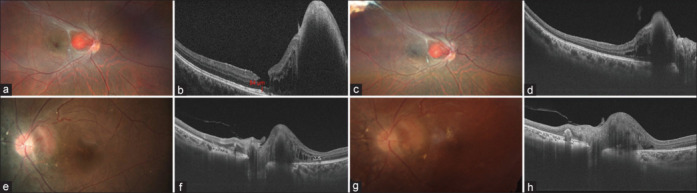
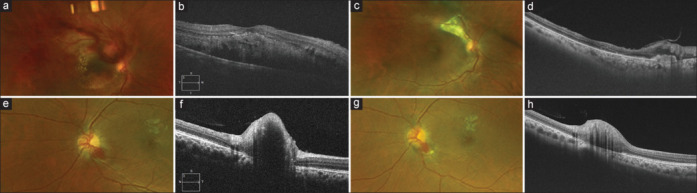
Methods: A prospective interventional case series. The technique involved ICG dye infusion 45 seconds prior to application of TTT. The main study outcomes were local tumor control, resolution of subretinal fluid (SRF), and improvement in best-corrected visual acuity (BCVA).
Results: Eight eyes of seven patients (5 males and 2 females) were included. The mean age was 26 years (range: 5-56 years). Systemic evaluation revealed von-Hippel Lindau (VHL) disease in five patients. The most common location was the temporal aspect of the optic disc (5 eyes). The mean basal diameter was 2.9 mm (range: 1-8 mm), and tumor thickness was 1.4 mm (range: 1-4 mm). All eight eyes were treated with multiple sessions of ICG-TTT (mean: 3 sessions). Six eyes received adjuvant intravitreal injection of dexamethasone implant (4 eyes) and/or bevacizumab (4 eyes). Post treatment, six eyes (75%) had tumor regression with reduction of SRF. One eye had a partial response with persisting SRF, and one eye showed poor response to TTT for which external beam radiotherapy was performed. At the last follow-up (median: 11 months; range: 6-29 months), the BCVA remained stable in seven eyes and improved in one eye (hand motion to 20/40).
Conclusion: Multiple ICG-TTT sessions can be considered as an alternative treatment option for JRCH with effective local tumor control and SRF resolution.
Copyright © 2024 Copyright: © 2024 Indian Journal of Ophthalmology.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Indocyanine Green-Enhanced Transpupillary Thermotherapy for Retinoblastoma: Analysis of 42 Tumors.J Pediatr Ophthalmol Strabismus. 2015 Nov-Dec;52(6):348-54. doi: 10.3928/01913913-20150929-17. J Pediatr Ophthalmol Strabismus. 2015. PMID: 26584748
-
Multimodal Imaging in the Diagnosis of Exophytic Juxtapapillary Retinal Capillary Hemangioblastoma.Am J Ophthalmol. 2021 May;225:128-136. doi: 10.1016/j.ajo.2021.01.002. Epub 2021 Jan 12. Am J Ophthalmol. 2021. PMID: 33450232
-
Photodynamic Therapy for Retinal Hemangioblastoma: Treatment Outcomes of 17 Consecutive Patients.Ophthalmol Retina. 2022 Jan;6(1):80-88. doi: 10.1016/j.oret.2021.04.007. Epub 2021 Apr 20. Ophthalmol Retina. 2022. PMID: 33892136
-
The effect of intravitreal bevacizumab and transpupillary thermotherapy on choroidal metastases and literature review.Indian J Ophthalmol. 2015 Jan;63(1):37-41. doi: 10.4103/0301-4738.151465. Indian J Ophthalmol. 2015. PMID: 25686061 Free PMC article. Review.
-
Fluorescein and indocyanine green angiography after transpupillary thermotherapy of choroidal neovascularization. Early vascular changes.Semin Ophthalmol. 2001 Jun;16(2):101-5. doi: 10.1076/soph.16.2.101.4209. Semin Ophthalmol. 2001. PMID: 15491012 Review.
Cited by
-
Vision-Threatening Complications of Juxtapapillary Retinal Capillary Hemangioma: A Case of Retinal Artery Occlusion.Am J Case Rep. 2025 Feb 20;26:e946514. doi: 10.12659/AJCR.946514. Am J Case Rep. 2025. PMID: 39972971 Free PMC article.
References
-
- Gass JD, Braunstein R. Sessile and exophytic capillary angiomas of the juxtapapillary retina and optic nerve head. Arch Ophthalmol. 1980;98:1790–7. - PubMed
-
- Singh AD, Shields CL, Shields JA. von Hippel-Lindau disease. Surv Ophthalmol. 2001;46:117–42. - PubMed
-
- Webster AR, Maher ER, Moore AT. Clinical characteristics of ocular angiomatosis in von Hippel-Lindau disease and correlation with germline mutation. Arch Ophthalmol. 1999;117:371–8. - PubMed
-
- Singh AD, Nouri M, Shields CL, Shields JA, Perez N. Treatment of retinal capillary hemangioma. Ophthalmology. 2002;109:1799–806. - PubMed
-
- Kreusel KM, Bechrakis NE, Krause L, Neumann HP, Foerster MH. Retinal angiomatosis in von Hippel-Lindau disease: A longitudinal ophthalmologic study. Ophthalmology. 2006;113:1418–24. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
