

Breaking the cycle of malaria treatment failure
- PMID: 38455307
- PMCID: PMC10910953
- DOI: 10.3389/fepid.2022.1041896
Breaking the cycle of malaria treatment failure
Abstract
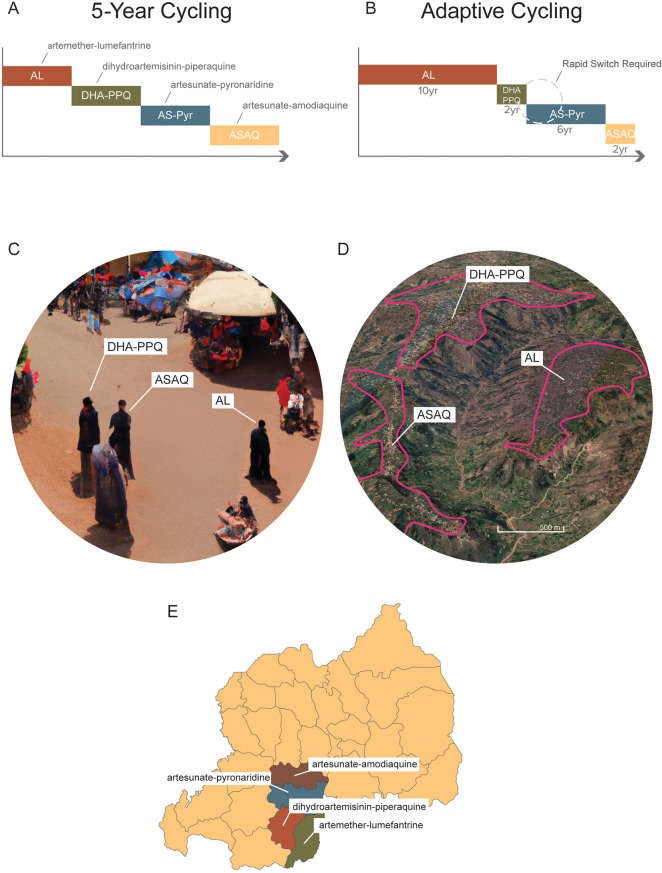
Treatment of symptomatic malaria became a routine component of the clinical and public health response to malaria after the second world war. However, all antimalarial drugs deployed against malaria eventually generated enough drug resistance that they had to be removed from use. Chloroquine, sulfadoxine-pyrimethamine, and mefloquine are well known examples of antimalarial drugs to which resistance did and still does ready evolve. Artemisinin-based combination therapies (ACTs) are currently facing the same challenge as artemisinin resistance is widespread in Southeast Asia and emerging in Africa. Here, I review some aspects of drug-resistance management in malaria that influence the strength of selective pressure on drug-resistant malaria parasites, as well as an approach we can take in the future to avoid repeating the common mistake of deploying a new drug and waiting for drug resistance and treatment failure to arrive. A desirable goal of drug-resistance management is to reduce selection pressure without reducing the overall percentage of patients that are treated. This can be achieved by distributing multiple first-line therapies (MFT) simultaneously in the population for the treatment of uncomplicated falciparum malaria, thereby keeping treatment levels high but the overall selection pressure exerted by each individual therapy low. I review the primary reasons that make MFT a preferred resistance management option in many malaria-endemic settings, and I describe two exceptions where caution and additional analyses may be warranted before deploying MFT. MFT has shown to be feasible in practice in many endemic settings. The continual improvement and increased coverage of genomic surveillance in malaria may allow countries to implement custom MFT strategies based on their current drug-resistance profiles.
Keywords: artemisinin combination therapies; artemisinin resistance; drug resistance; malaria; multiple first-line therapies.
© 2022 Boni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Combined antimalarial therapy using artemisinin].Parassitologia. 2004 Jun;46(1-2):85-7. Parassitologia. 2004. PMID: 15305693 Review. Italian.
-
Malaria Surveillance - United States, 2018.MMWR Surveill Summ. 2022 Sep 2;71(8):1-35. doi: 10.15585/mmwr.ss7108a1. MMWR Surveill Summ. 2022. PMID: 36048717 Free PMC article.
-
Antimalarial drug resistance in Africa: key lessons for the future.Ann N Y Acad Sci. 2015 Apr;1342:62-7. doi: 10.1111/nyas.12766. Ann N Y Acad Sci. 2015. PMID: 25891142 Free PMC article. Review.
-
Malaria Surveillance - United States, 2016.MMWR Surveill Summ. 2019 May 17;68(5):1-35. doi: 10.15585/mmwr.ss6805a1. MMWR Surveill Summ. 2019. PMID: 31099769
-
Response of falciparum malaria to different antimalarials in Myanmar.Bull World Health Organ. 1999;77(3):244-9. Bull World Health Organ. 1999. PMID: 10212515 Free PMC article. Clinical Trial.
Cited by
-
Antimalarial mass drug administration in large populations and the evolution of drug resistance.PLOS Glob Public Health. 2023 Jul 26;3(7):e0002200. doi: 10.1371/journal.pgph.0002200. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37494337 Free PMC article.
-
Plasmodium falciparum multidrug resistance 1 gene polymorphisms associated with outcomes after anti-malarial treatment.Malar J. 2025 Jun 12;24(1):186. doi: 10.1186/s12936-025-05248-2. Malar J. 2025. PMID: 40506728 Free PMC article.
-
Geospatial Analysis of Malaria Burden in Kagera Region, Northwestern Tanzania Using Health Facility and Community Survey Data.Open Forum Infect Dis. 2024 Oct 11;11(11):ofae609. doi: 10.1093/ofid/ofae609. eCollection 2024 Nov. Open Forum Infect Dis. 2024. PMID: 39507880 Free PMC article.
-
Global risk of selection and spread of Plasmodium falciparum histidine-rich protein 2 and 3 gene deletions.medRxiv [Preprint]. 2024 Jan 1:2023.10.21.23297352. doi: 10.1101/2023.10.21.23297352. medRxiv. 2024. PMID: 37905102 Free PMC article. Preprint.
-
Preventing antimalarial drug resistance with triple artemisinin-based combination therapies.Nat Commun. 2023 Jul 29;14(1):4568. doi: 10.1038/s41467-023-39914-3. Nat Commun. 2023. PMID: 37516752 Free PMC article.
References
LinkOut - more resources
Full Text Sources