

Assessing Intra-abdominal status for clinically relevant postoperative pancreatic fistula based on postoperative fluid collection and drain amylase levels after distal pancreatectomy
- PMID: 38455495
- PMCID: PMC10914692
- DOI: 10.1002/ags3.12741
Assessing Intra-abdominal status for clinically relevant postoperative pancreatic fistula based on postoperative fluid collection and drain amylase levels after distal pancreatectomy
Abstract
Aim: The aim of this study was to evaluate the intra-abdominal status related to postoperative pancreatic fistula by combining postoperative fluid collection and drain amylase levels.
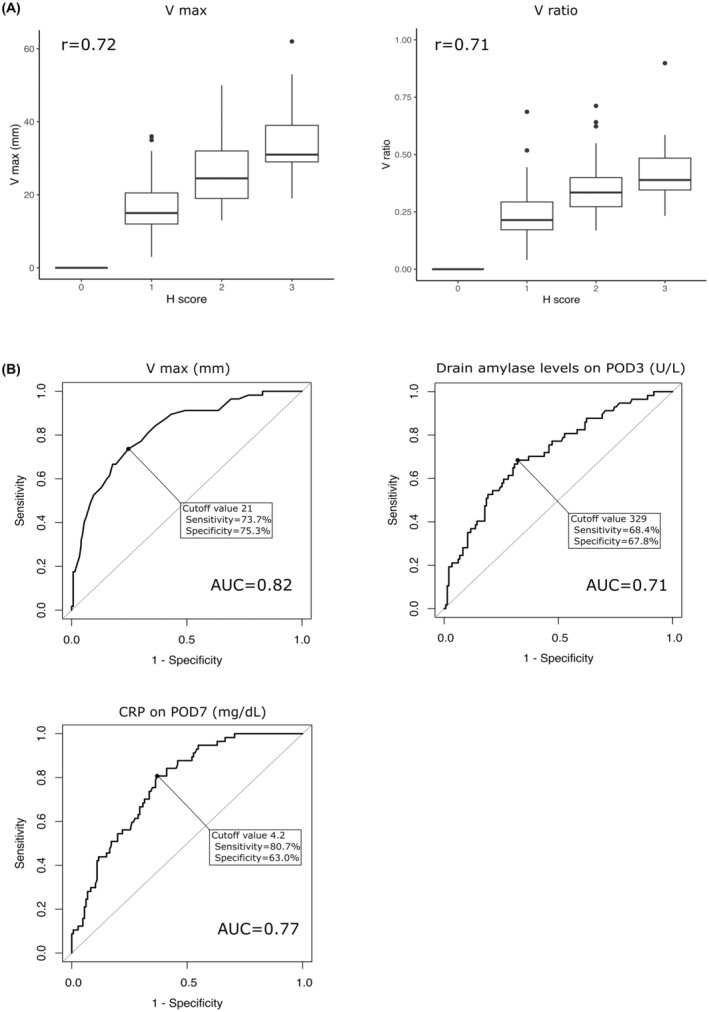
Methods: We retrospectively reviewed the data of 203 patients who underwent distal pancreatectomy and classified their postoperative abdominal status into four groups based on postoperative fluid collection size and drain amylase levels. We also evaluated the incidence of clinically relevant postoperative pancreatic fistula in each group according to C-reactive protein values.
Results: The incidence of clinically relevant postoperative pancreatic fistula in the entire cohort (n = 203) was 28.1%. Multivariate analysis revealed that postoperative fluid collection, drain amylase levels, and C-reactive protein levels are considerable risk factors for clinically relevant postoperative pancreatic fistula. In the subgroup with large postoperative fluid collection and high drain amylase levels, 65.9% of patients developed clinically relevant postoperative pancreatic fistula. However, no significant difference was observed in C-reactive protein levels between patients with clinically relevant postoperative pancreatic fistula and those without it. In contrast, in the subgroup with a large postoperative fluid collection size or a high amylase level alone, a significant difference was observed in C-reactive protein values between the patients with clinically relevant postoperative pancreatic fistula and those without it.
Conclusion: Postoperative fluid collection status and the C-reactive protein value provide a more precise assessment of intra=abdominal status related to postoperative pancreatic fistula after distal pancreatectomy. This detailed analysis may be a clinically reasonable approach to individual drain management.
Keywords: amylase; analysis; pancreatectomy; pancreatic fistula; patients.
© 2023 The Authors. Annals of Gastroenterological Surgery published by John Wiley & Sons Australia, Ltd on behalf of The Japanese Society of Gastroenterological Surgery.
Conflict of interest statement
The authors declare no conflicts of interest for this article.
Figures


References
-
- Pannegeon V, Pessaux P, Sauvanet A, Vullierme MP, Kianmanesh R, Belghiti J. Pancreatic fistula after distal pancreatectomy: predictive risk factors and value of conservative treatment. Arch Surg. 2006;141(11):1071–1076. - PubMed
-
- Hackert T, Werner J, Büchler MW. Postoperative pancreatic fistula. Surgeon. 2011;9(4):211–217. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
