

Familial pulmonary cysts: A clue to diagnose Birt-Hogg-Dubé syndrome: A case report and literature review
- PMID: 38455502
- PMCID: PMC10918712
- DOI: 10.1002/rcr2.1319
Familial pulmonary cysts: A clue to diagnose Birt-Hogg-Dubé syndrome: A case report and literature review
Abstract
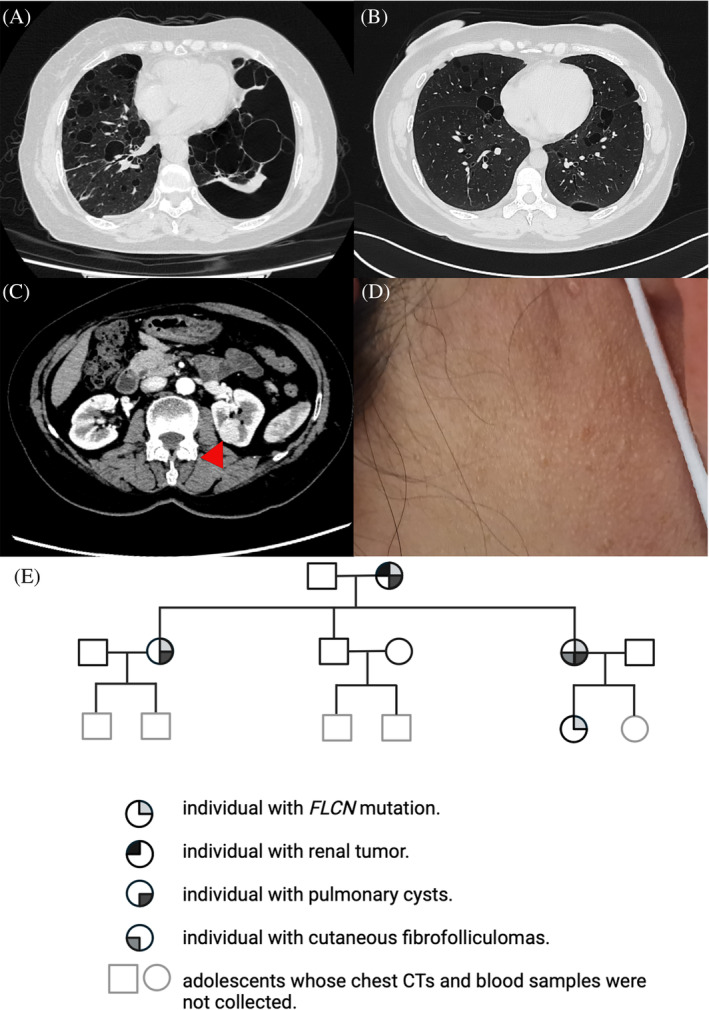
Birt-Hogg-Dubé syndrome (BHD) is an inherited autosomal dominant condition caused by germline mutations in the FLCN gene, mapped to chromosome 17p11.2. Typical manifestations include pulmonary cysts, spontaneous pneumothorax, fibrofolliculomas, and kidney neoplasms. This report details the case of a 56-year-old female non-smoker diagnosed with multiple pulmonary cysts, presenting with a history of recurrent spontaneous pneumothorax. A computed tomography (CT) scan of her daughter revealed similar pulmonary cysts, raising suspicion of BHD. Further abdominal enhanced CT revealed a left renal tumour and cutaneous fibrofolliculomas on her daughter's neck. Consequently, whole-exome sequencing confirmed an FLCN germline mutation in the patient and three relatives, establishing a diagnosis of BHD. This case highlights the importance of familial pulmonary cysts as a clue for diagnosing BHD, providing crucial insights into comparable clinical presentations.
Keywords: Birt–Hogg–Dubé syndrome; FLCN gene; familial pulmonary cysts.
© 2024 The Authors. Respirology Case Reports published by John Wiley & Sons Australia, Ltd on behalf of The Asian Pacific Society of Respirology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
[Expert consensus on the diagnosis and management of Birt-Hogg-Dubé syndrome].Zhonghua Jie He He Hu Xi Za Zhi. 2023 Sep 12;46(9):897-908. doi: 10.3760/cma.j.cn112147-20230705-00362. Zhonghua Jie He He Hu Xi Za Zhi. 2023. PMID: 37670643 Chinese.
-
Spontaneous Pneumothorax Diagnosed As Birt-Hogg-Dubé Syndrome: A Report of a Rare Case.Cureus. 2025 Mar 1;17(3):e79875. doi: 10.7759/cureus.79875. eCollection 2025 Mar. Cureus. 2025. PMID: 40166800 Free PMC article.
-
Birt-Hogg-Dubé syndrome.Eur Respir Rev. 2020 Sep 17;29(157):200042. doi: 10.1183/16000617.0042-2020. Print 2020 Sep 30. Eur Respir Rev. 2020. PMID: 32943413 Free PMC article.
-
Birt-Hogg-Dubé syndrome: a literature review and case study of a Chinese woman presenting a novel FLCN mutation.BMC Pulm Med. 2017 Feb 21;17(1):43. doi: 10.1186/s12890-017-0383-9. BMC Pulm Med. 2017. PMID: 28222720 Free PMC article. Review.
-
Birt-Hogg-Dubé syndrome associated with chorioretinopathy and nyctalopia: a case report and review of the literature.Ophthalmic Genet. 2023 Apr;44(2):175-181. doi: 10.1080/13816810.2021.1961281. Epub 2021 Aug 6. Ophthalmic Genet. 2023. PMID: 34353225 Review.
References
-
- Menko FH, van Steensel MA, Giraud S, et al. Birt‐Hogg‐Dubé syndrome: diagnosis and management. Lancet Oncol. 2009;10(12):1199–1206. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
