

Symptomatic Pneumonitis With Durvalumab After Concurrent Chemoradiotherapy in Unresectable Stage III NSCLC
- PMID: 38455595
- PMCID: PMC10918565
- DOI: 10.1016/j.jtocrr.2024.100638
Symptomatic Pneumonitis With Durvalumab After Concurrent Chemoradiotherapy in Unresectable Stage III NSCLC
Abstract
Introduction: In the placebo-controlled, phase 3 PACIFIC trial, durvalumab significantly prolonged progression-free survival (PFS) (p < 0.0001) and overall survival (OS) (p = 0.00251) in patients with unresectable stage III NSCLC and no progression after platinum-based concurrent chemoradiotherapy (cCRT). Pneumonitis or radiation pneumonitis (PRP) was common in both arms. We report exploratory analyses evaluating the association of symptomatic (grade ≥2) PRP (G2+PRP) with baseline factors and clinical outcomes.
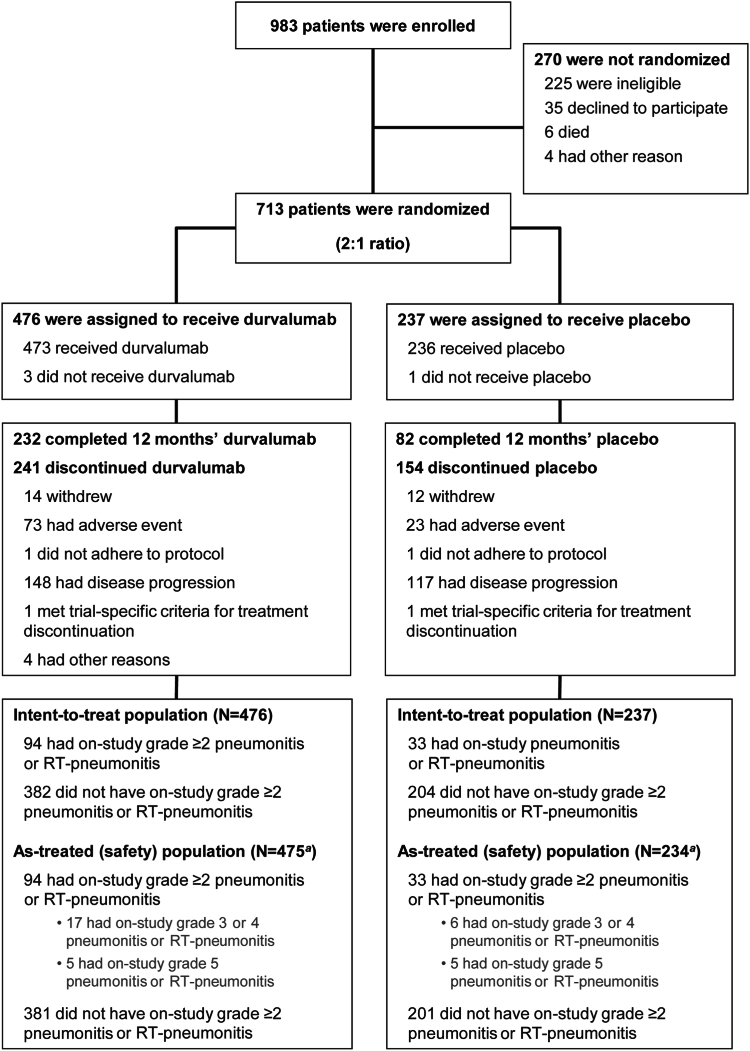
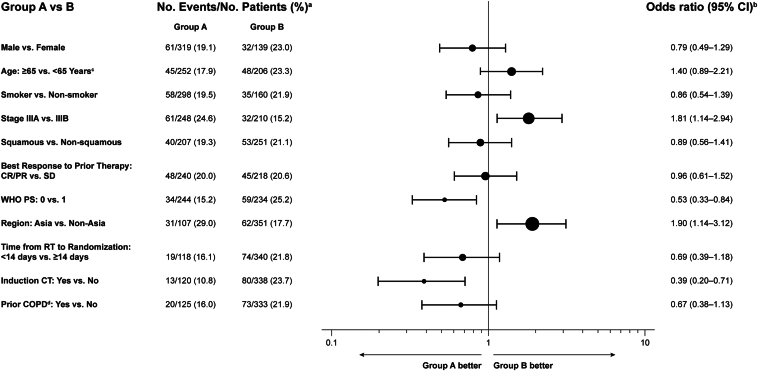
Methods: Patients with WHO performance status of 0 or 1 were randomized (2:1) to 12 months of durvalumab or placebo, 1 to 42 days after cCRT. Associations between baseline factors and on-study G2+PRP in durvalumab-treated patients were investigated using univariate and multivariate logistic regression. PFS and OS were analyzed using Cox proportional hazards models adjusted for time-dependent G2+PRP plus covariates for randomization stratification factors without and with additional baseline factors.
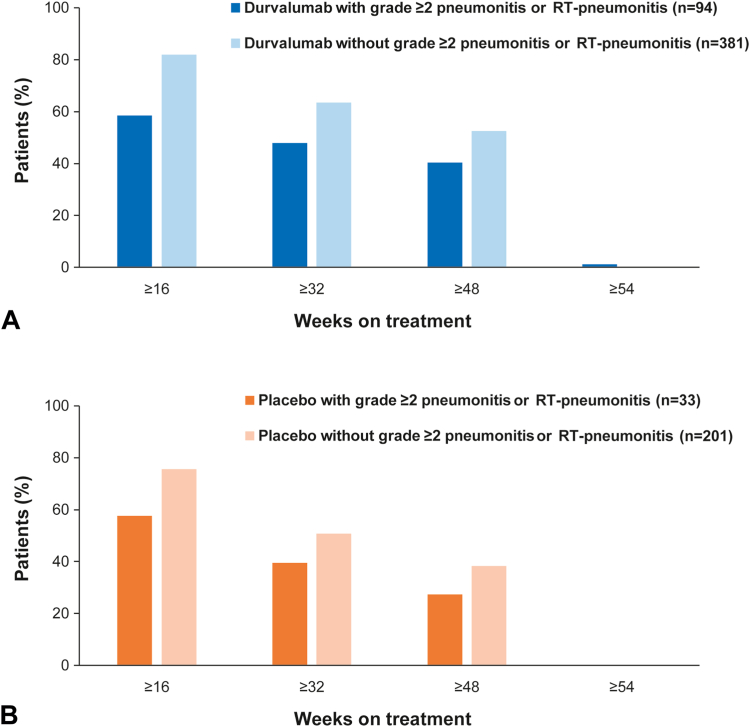
Results: On-study G2+PRP occurred in 94 of 475 (19.8%) and 33 of 234 patients (14.1%) on durvalumab and placebo, respectively (median follow-up, 25.2 mo); grade greater than or equal to 3 PRP was uncommon (4.6% and 4.7%, respectively). Time to onset and resolution of G2+PRP was similar with durvalumab and placebo. Univariate and multivariate analyses identified patients treated in Asia, those with stage IIIA disease, those with performance status of 1, and those who had not received induction chemotherapy as having a higher risk of G2+PRP. PFS and OS benefit favoring durvalumab versus placebo was maintained regardless of time-dependent G2+PRP.
Conclusions: Factors associated with higher risk of G2+PRP with durvalumab after cCRT were identified. Clinical benefit was maintained regardless of on-study G2+PRP, suggesting the risk of this event should not deter the use of durvalumab in eligible patients with unresectable stage III NSCLC.
Keywords: Durvalumab; Immunotherapy; Locally advanced NSCLC; Pulmonary toxicity; Radiotherapy.
© 2024 The Authors.
Conflict of interest statement
Dr. Vansteenkiste reports receiving institutional research funding from 10.13039/100009947Merck Sharp & Dohme; receiving advisory, consulting fees from AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, and Roche; receiving payment or honoraria from Merck, Merck Sharp & Dohme, and Sanofi; having participation on a data safety monitoring or advisory board from PDCline, Daiichi Sankyo, and Boehringer Ingelheim; and having a leadership role in the Lung Education Group for European Society for Medical Oncology (ESMO). Prof. Naidoo reports receiving institutional research funding from 10.13039/100004325AstraZeneca, 10.13039/100002491Bristol-Myers Squibb, 10.13039/100004337Roche/10.13039/100004328Genentech, 10.13039/100002429Amgen, Mirati, 10.13039/100004319Pfizer, 10.13039/100008373Takeda, and 10.13039/100004336Novartis; advisory and/or consulting fees from AstraZeneca, Bristol-Myers Squibb, Takeda, Pfizer, Daiichi Sankyo, Roche/Genentech, Kaleido Biosciences, Amgen, Novartis, NGM Pharmaceuticals, Elevation Oncology, and Mirati; honoraria from AstraZeneca, Bristol-Myers Squibb, Takeda, Pfizer, Daiichi Sankyo, Roche/Genentech, Kaleido Biosciences, Amgen, Novartis, NGM Pharmaceuticals, Elevation Oncology, and Mirati; support for attending meetings from AstraZeneca and Roche/Genentech; and having participation on a data safety monitoring or advisory board for Bristol-Myers Squibb, AstraZeneca, and Daiichi Sankyo. Prof. Faivre-Finn reports receiving institutional research funding from AstraZeneca, Merck Sharp & Dohme, and Elekta; institutional consulting fees, honoraria, and support for attending meetings and/or travel from AstraZeneca and Merck Sharp & Dohme; and having participation on a data safety monitoring or advisory board from AstraZeneca and Merck Sharp & Dohme/Merck. Dr. Villegas reports receiving honoraria and support for attending meetings and/or travel from AstraZeneca. Dr. Daniel reports receiving institutional research funding from Genentech, Roche, Celgene, Guardant, Janssen, Bristol-Myers Squibb, Merck, Novartis, AbbVie, ARMO Biosciences, Lilly Merus, Daiichi Sankyo, EQRX, and G1 Therapeutics; is a member of the Board of Directors for the Common Spirit Memorial Hospital Board, and the Board of Governors for Tennessee Oncology. Dr. Murakami reports receiving institutional research funding from AstraZeneca, Takeda, Hugai Pharma, Sanofi, Merck Sharp & Dohme, Daiichi Sankyo, Ono Pharmaceutical, and Janssen Pharma; honoraria from AstraZeneca, Chugai Pharma, Takeda, Eli Lilly, Merck Sharp & Dohme, Pfizer, Novartis, and Taiho Pharmaceutical. Dr. Hui reports receiving institutional research funding from AstraZeneca, 10.13039/501100003769Eisai, Eli Lilly, 10.13039/100005565Janssen, 10.13039/100009947Merck Sharp & Dohme, 10.13039/100004336Novartis, 10.13039/100019104OncoSec, Roche, and 10.13039/100020124Seagen; payment or honoraria from AstraZeneca, Eli Lilly, Janssen, Merck Sharp & Dohme, Novartis, and Roche; having participation on an advisory board for Amgen, AstraZeneca, Bristol-Myers Squibb, Eisai, Eli Lilly, Merck, Merck Sharp & Dohme, Novartis, Oncosec, Pfizer, Roche, Seagen, Takeda, and Zai Lab; and having a leadership or fiduciary role in the ESMO Congress 2021 Scientific Committee, the ESMO Congress 2022 Scientific Committee, and the International Association for the Study of Lung Cancer Education Committee. Dr. Lee reports having participation on an advisory board for Bristol-Myers Squibb, Merck Sharp & Dohme, Pfizer, AstraZeneca, and Eli Lilly; and receipt of study drugs from Merck. Dr. Cho reports receiving institutional research funding from MOGAM Institute, 10.13039/501100020430LG Chem, Oscotec, Interpark Bio Convergence Corp., GIInnovation, GI-Cell, Abion, AbbVie, AstraZeneca, 10.13039/100004326Bayer, Blueprint Medicines, Boehringer Ingelheim, 10.13039/100020838Champions Oncology, CJ Bioscience, CJ Blossom Park, Cyrus, Dizal Pharma, Genexine, 10.13039/100005565Janssen, 10.13039/100020536Lilly, Merck Sharp & Dohme, Novartis, Nuvalent, Oncternal, Ono, 10.13039/100009857Regeneron, Dong-A ST, Bridgebio Therapeutics, 10.13039/100019265Yuhan, ImmuneOncia, 10.13039/100010905Illumina, Kanaph Therapeutics, Therapex, JINTSbio, Hanmi, and CHA Bundang Medical Center; royalties from Champions Oncology, Crown Bioscience, and Imagen; consulting fees from Abion, BeiGene, Novartis, AstraZeneca, Boehringer Ingelheim, Roche, Bristol-Myers Squibb, CJ, CureLogen, Cyrus Therapeutics, Ono, Onegene Biotechnology, Yuhan, Pfizer, Eli Lilly, GI-Cell, Guardant, HK Inno-N, Imnewrun Biosciences Inc., Janssen, Takeda, Merck Sharp & Dohme, Janssen, Medpacto, Blueprint Medicines, RandBio, and Hanmi; payment or honoraria from American Society of Clinical Oncology, AstraZeneca, Guardant, Roche, ESMO, International Association for the Study of Lung Cancer, Korean Cancer Association, Korean Society of Medical Oncology, Korean Society of Thyroid-Head and Neck Surgery, Korean Cancer Study Group, Novartis, Merck Sharp & Dohme, The Chinese Thoracic Oncology Society, and Pfizer; membership on a Scientific Advisory Board for Kanaph Therapeutic Inc., Bridgebio Therapeutics, Cyrus Therapeutics, Guardant Health, and Oscotec Inc.; membership on the Board of Directors for Interpark Bio Convergence Corp. and J INTS BIO; stock ownership in TheraCanVac, Inc., Gencurix Inc., Bridgebio Therapeutics, Kanaph Therapeutic Inc., Cyrus Therapeutics, Interpark Bio Convergence Corp., and J INTS BIO; employment by the Yonsei University Health System; and is a founder of DAAN Biotherapeutics. Dr. Kubota reports receiving research funding from AstraZeneca; payment or honoraria from AstraZeneca, Merck Sharp & Dohme, Merck, Ono, Chugai, Taiho, Kyowa-Kirin, Bristol-Myers Squibb, Novartis, Eli Lilly, Pfizer, Nihon-Kayaku, and BIH; and a leadership or fiduciary role for the Japan Multi-National Trial Organization, Japan Clinical Oncology Group, Thoracic Oncology Research Group, North East Japan Study Group, and Japan Association of Medical Translation for Cancer. Ms. Broadhurst reports receiving consulting fees from AstraZeneca, employment with AstraZeneca (under contract from Plus-Project Ltd.), and stock ownership in AstraZeneca. Ms. Wadsworth, Dr. Newton, and Dr. Thiyagarajah report employment and stock ownership in AstraZeneca. Dr. Antonia reports research funding from AstraZeneca and 10.13039/100009857Regeneron; consulting and/or scientific advisory board fees from Memgen, RAPT Biotherapeutics, Achilles Therapeutics, Xilis, Taurus Therapeutics, Shoreline Therapeutics, Immutep, and Leap Therapeutics; royalties or licenses from H. Lee Moffitt Cancer Center; stock ownership in Shoreline Therapeutics, Leap Therapeutics, RAPT Biotherapeutics, and Achilles Therapeutics; receipt of drug supply for a clinical trial from Amgen; and support for attending meetings and/or travel from Achilles Therapeutics and RAPT Biotherapeutics. Dr. Özgüroğlu reports no disclosures.
Figures
References
-
- Postmus P.E., Kerr K.M., Oudkerk M., et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl 4):IV1–IV21. - PubMed
-
- Bradley J.D., Paulus R., Komaki R., et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015;16:187–199. - PMC - PubMed
-
- Senan S., Brade A., Wang L., et al. PROCLAIM: a randomized, phase III trial of pemetrexed-cisplatin or etoposide-cisplatin plus thoracic radiation therapy followed by consolidation chemotherapy in locally advanced non-squamous non-small cell lung cancer. J Clin Oncol. 2016;34:953–962. - PubMed
-
- Antonia S.J., Villegas A., Daniel D., et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Eng J Med. 2017;377:1919–1929. - PubMed
-
- Antonia S.J., Villegas A., Daniel D., et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N Eng J Med. 2018;379:2342–2350. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
