

Progress Note 2024: Curing HIV; Not in My Lifetime or Just Around the Corner?
- PMID: 38455668
- PMCID: PMC10919397
- DOI: 10.20411/pai.v8i2.665
Progress Note 2024: Curing HIV; Not in My Lifetime or Just Around the Corner?
Erratum in
-
Erratum to: Progress Note 2024: Curing HIV; Not in My Lifetime or Just Around the Corner?Pathog Immun. 2024 Mar 12;8(2):179-222. doi: 10.20411/pai.v8i2.696. eCollection 2023. Pathog Immun. 2024. PMID: 38505662 Free PMC article.
Abstract
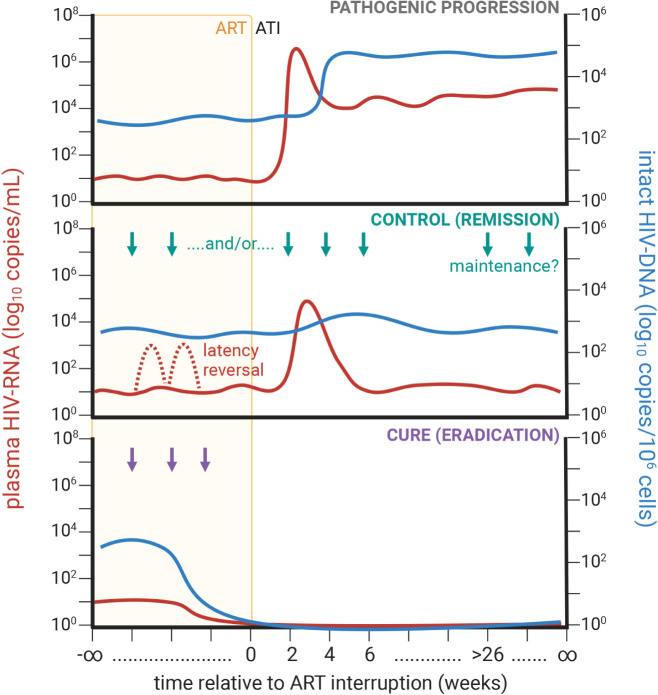
Once a death sentence, HIV is now considered a manageable chronic disease due to the development of antiretroviral therapy (ART) regimens with minimal toxicity and a high barrier for genetic resistance. While highly effective in arresting AIDS progression and rendering the virus untransmissible in people living with HIV (PLWH) with undetectable viremia (U=U) [1, 2]), ART alone is incapable of eradicating the "reservoir" of resting, latently infected CD4+ T cells from which virus recrudesces upon treatment cessation. As of 2022 estimates, there are 39 million PLWH, of whom 86% are aware of their status and 76% are receiving ART [3]. As of 2017, ART-treated PLWH exhibit near normalized life expectancies without adjustment for socioeconomic differences [4]. Furthermore, there is a global deceleration in the rate of new infections [3] driven by expanded access to pre-exposure prophylaxis (PrEP), HIV testing in vulnerable populations, and by ART treatment [5]. Therefore, despite outstanding issues pertaining to cost and access in developing countries, there is strong enthusiasm that aggressive testing, treatment, and effective viral suppression may be able to halt the ongoing HIV epidemic (ie, UNAIDS' 95-95-95 targets) [6-8]; especially as evidenced by recent encouraging observations in Sydney [9]. Despite these promising efforts to limit further viral transmission, for PLWH, a "cure" remains elusive; whether it be to completely eradicate the viral reservoir (ie, cure) or to induce long-term viral remission in the absence of ART (ie, control; Figure 1). In a previous salon hosted by Pathogens and Immunity in 2016 [10], some researchers were optimistic that a cure was a feasible, scalable goal, albeit with no clear consensus on the best route. So, how are these cure strategies panning out? In this commentary, 8 years later, we will provide a brief overview on recent advances and failures towards identifying determinants of viral persistence and developing a scalable cure for HIV. Based on these observations, and as in the earlier salon, we have asked several prominent HIV cure researchers for their perspectives.
Keywords: ART; HIV; HIV control; HIV cure; SIV; persistence; reservoir.
Copyright © 2024 Pathogens and Immunity.
Conflict of interest statement
JH and MP have active collaborations with Merck & Co., Inc., and routinely receive antiretroviral compounds for nonhuman primate studies from ViiV Healthcare and Gilead Sciences, but the authors declare no financial stake. MML has received competitive grant funding from Gilead.
Figures
Similar articles
-
A Cure for HIV Infection: "Not in My Lifetime" or "Just Around the Corner"?Pathog Immun. 2016 Spring;1(1):154-164. doi: 10.20411/pai.v1i1.133. Pathog Immun. 2016. PMID: 27668293 Free PMC article.
-
Brain Macrophages in Simian Immunodeficiency Virus-Infected, Antiretroviral-Suppressed Macaques: a Functional Latent Reservoir.mBio. 2017 Aug 15;8(4):e01186-17. doi: 10.1128/mBio.01186-17. mBio. 2017. PMID: 28811349 Free PMC article.
-
Antibody-Mediated CD4 Depletion Induces Homeostatic CD4+ T Cell Proliferation without Detectable Virus Reactivation in Antiretroviral Therapy-Treated Simian Immunodeficiency Virus-Infected Macaques.J Virol. 2018 Oct 29;92(22):e01235-18. doi: 10.1128/JVI.01235-18. Print 2018 Nov 15. J Virol. 2018. PMID: 30185596 Free PMC article.
-
Reservoirs for HIV-1: mechanisms for viral persistence in the presence of antiviral immune responses and antiretroviral therapy.Annu Rev Immunol. 2000;18:665-708. doi: 10.1146/annurev.immunol.18.1.665. Annu Rev Immunol. 2000. PMID: 10837072 Review.
-
Pediatric HIV: the Potential of Immune Therapeutics to Achieve Viral Remission and Functional Cure.Curr HIV/AIDS Rep. 2020 Jun;17(3):237-248. doi: 10.1007/s11904-020-00495-1. Curr HIV/AIDS Rep. 2020. PMID: 32356090 Free PMC article. Review.
Cited by
-
Safety, pharmacokinetics, and biological activity of CD4-mimetic BNM-III-170 in SHIV-infected rhesus macaques.J Virol. 2025 May 20;99(5):e0006225. doi: 10.1128/jvi.00062-25. Epub 2025 Apr 7. J Virol. 2025. PMID: 40192306 Free PMC article.
-
"This Is How I Give Back": Long-Term Survivors on Legacy and HIV Cure Research at the End of Life-A Qualitative Inquiry in the United States.Infect Dis Rep. 2025 Jul 4;17(4):78. doi: 10.3390/idr17040078. Infect Dis Rep. 2025. PMID: 40700324 Free PMC article.
References
-
- Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, Hakim JG, Kumwenda J, Grinsztejn B, Pilotto JH, Godbole SV, Chariyalertsak S, Santos BR, Mayer KH, Hoffman IF, Eshleman SH, Piwowar-Manning E, Cottle L, Zhang XC, Makhema J, Mills LA, Panchia R, Faesen S, Eron J, Gallant J, Havlir D, Swindells S, Elharrar V, Burns D, Taha TE, Nielsen-Saines K, Celentano DD, Essex M, Hudelson SE, Redd AD, Fleming TR, Team HS. Antiretroviral Therapy for the Prevention of HIV-1 Transmission. N Engl J Med. 2016;375(9):830–9. Epub 20160718. doi: 10.1056/NEJMoa1600693. PubMed PMID: 27424812; PMCID: PMC5049503. - DOI - PMC - PubMed
-
- Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, Degen O, Corbelli GM, Estrada V, Geretti AM, Beloukas A, Raben D, Coll P, Antinori A, Nwokolo N, Rieger A, Prins JM, Blaxhult A, Weber R, Van Eeden A, Brockmeyer NH, Clarke A, Del Romero Guerrero J, Raffi F, Bogner JR, Wandeler G, Gerstoft J, Gutierrez F, Brinkman K, Kitchen M, Ostergaard L, Leon A, Ristola M, Jessen H, Stellbrink HJ, Phillips AN, Lundgren J, Group PS. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet. 2019;393(10189):2428–38. Epub 20190502. doi: 10.1016/S0140-6736(19)30418-0. PubMed PMID: 31056293; PMCID: PMC6584382. - DOI - PMC - PubMed
-
- UNAIDS. Global HIV & AIDS statistics — Fact sheet 2022 [cited 2023 October 2]. Available from: https://www.unaids.org/en/resources/fact-sheet.
-
- Edwards JK, Cole SR, Breger TL, Rudolph JE, Filiatreau LM, Buchacz K, Humes E, Rebeiro PF, D'Souza G, Gill MJ, Silverberg MJ, Mathews WC, Horberg MA, Thorne J, Hall HI, Justice A, Marconi VC, Lima VD, Bosch RJ, Sterling TR, Althoff KN, Moore RD, Saag M, Eron JJ. Mortality Among Persons Entering HIV Care Compared With the General U.S. Population : An Observational Study. Ann Intern Med. 2021;174(9):1197–206. Epub 20210706. doi: 10.7326/M21-0065. PubMed PMID: 34224262; PMCID: PMC8453103. - DOI - PMC - PubMed
-
- Center for Disease Control and Prevention. HIV Declines Among Young People and Drives Overall Decrease in New HIV Infections [cited 2023 October 2]. Available from: https://www.cdc.gov/media/releases/2023/p0523-hiv-declines-among-young-p....
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous