

Pain, comorbidities, and clinical decision-making: conceptualization, development, and pilot testing of the Pain in Aging, Educational Assessment of Need instrument
- PMID: 38455875
- PMCID: PMC10918012
- DOI: 10.3389/fpain.2024.1254792
Pain, comorbidities, and clinical decision-making: conceptualization, development, and pilot testing of the Pain in Aging, Educational Assessment of Need instrument
Abstract
Introduction: Pain is highly prevalent in older adults and often contextualized by multiple clinical conditions (pain comorbidities). Pain comorbidities increase with age and this makes clinical decisions more complex. To address gaps in clinical training and geriatric pain management, we established the Pain in Aging-Educational Assessment of Need (PAEAN) project to appraise the impacts of medical and mental health conditions on clinical decision-making regarding older adults with pain. We here report development and pilot testing of the PAEAN survey instrument to assess clinician perspectives.
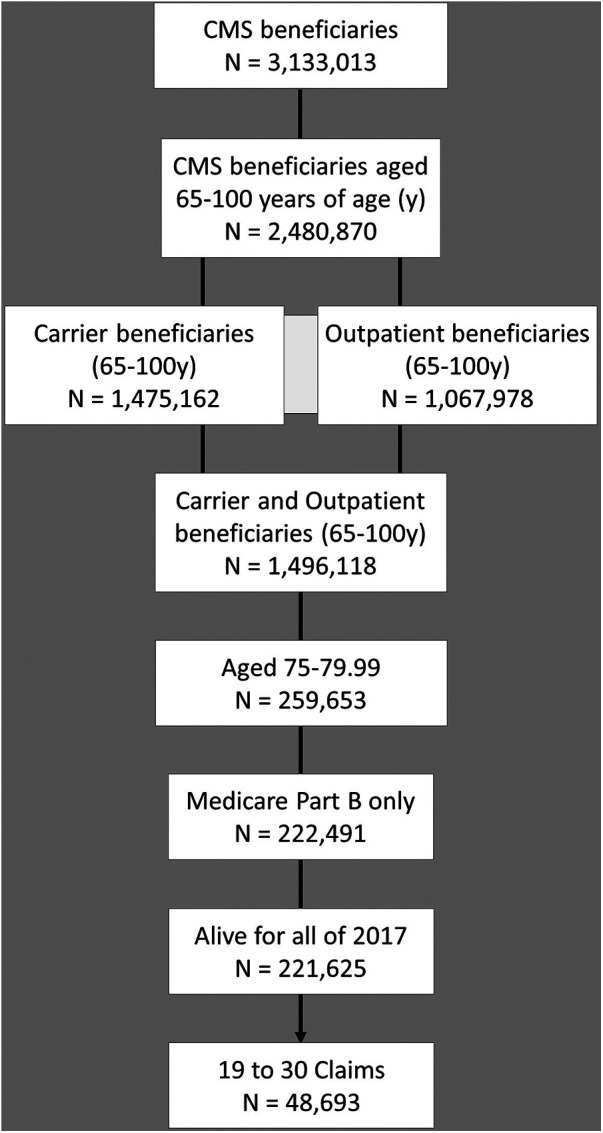
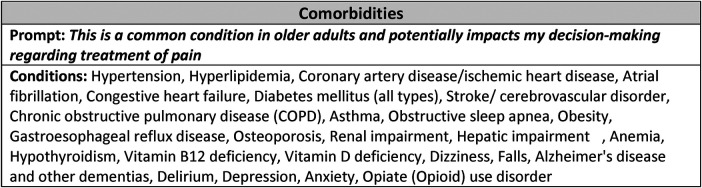
Methods: Mixed-methods approaches were used. Scoping review methodology was applied to appraise both research literature and selected Medicare-based data. A geographically and professionally diverse interprofessional advisory panel of experts in pain research, medical education, and geriatrics was formed to advise development of the list of pain comorbidities potentially impacting healthcare professional clinical decision-making. A survey instrument was developed, and pilot tested by diverse licensed healthcare practitioners from 2 institutions. Respondents were asked to rate agreement regarding clinical decision-making impact using a 5-point Likert scale. Items were scored for percent agreement.
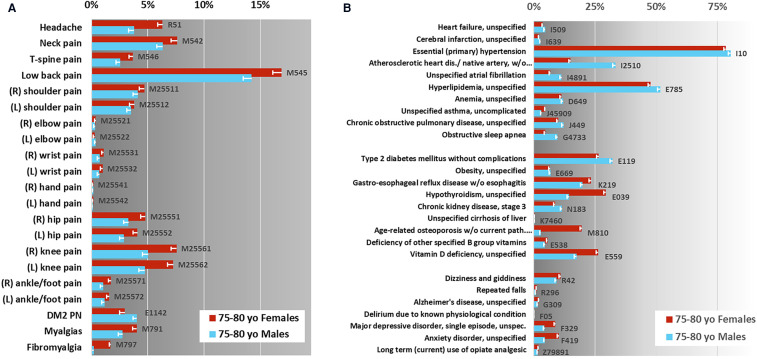
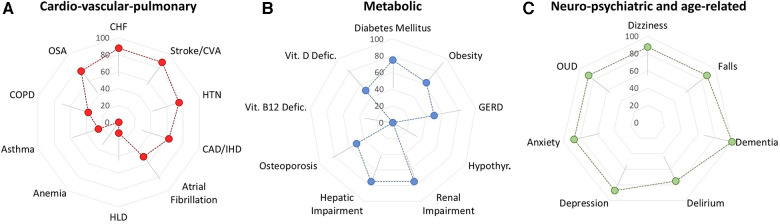
Results: Scoping reviews indicated that pain conditions and comorbidities are prevalent in older adults but not universally recognized. We found no research literature directly guiding pain educators in designing pain education modules that mirror older adult clinical complexity. The interprofessional advisory panel identified 26 common clinical conditions for inclusion in the pilot PAEAN instrument. Conditions fell into three main categories: "major medical", i.e., cardio-vascular-pulmonary; metabolic; and neuropsychiatric/age-related. The instrument was pilot tested by surveying clinically active healthcare providers, e.g., physicians, nurse practitioners, who all responded completely. Median survey completion time was less than 3 min.
Conclusion: This study, developing and pilot testing our "Pain in Aging-Educational Assessment of Need" (PAEAN) instrument, suggests that 1) many clinical conditions impact pain clinical decision-making, and 2) surveying healthcare practitioners about the impact of pain comorbidities on clinical decision-making for older adults is highly feasible. Given the challenges intrinsic to safe and effective clinical care of older adults with pain, and attendant risks, together with the paucity of existing relevant work, much more education and research are needed.
Keywords: chronic pain; clinical decision-making; geriatric; interdisciplinary; interprofessional; multimorbidity; pain education; survey instrument.
© 2024 Siaton, Hogans, Frey-Law, Brown, Herndon and Buenaver.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The handling editor JWW declared a past collaboration with one of the authors BH.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources