

Outcomes and efficacy of magnetic resonance imaging-compatible sacral nerve stimulator for management of fecal incontinence: A multi-institutional study
- PMID: 38455883
- PMCID: PMC10915907
- DOI: 10.4329/wjr.v16.i2.32
Outcomes and efficacy of magnetic resonance imaging-compatible sacral nerve stimulator for management of fecal incontinence: A multi-institutional study
Abstract
Background: Fecal incontinence (FI) is an involuntary passage of fecal matter which can have a significant impact on a patient's quality of life. Many modalities of treatment exist for FI. Sacral nerve stimulation is a well-established treatment for FI. Given the increased need of magnetic resonance imaging (MRI) for diagnostics, the InterStim which was previously used in sacral nerve stimulation was limited by MRI incompatibility. Medtronic MRI-compatible InterStim was approved by the United States Food and Drug Administration in August 2020 and has been widely used.
Aim: To evaluate the efficacy, outcomes and complications of the MRI-compatible InterStim.
Methods: Data of patients who underwent MRI-compatible Medtronic InterStim placement at UPMC Williamsport, University of Minnesota, Advocate Lutheran General Hospital, and University of Wisconsin-Madison was pooled and analyzed. Patient demographics, clinical features, surgical techniques, complications, and outcomes were analyzed. Strengthening the Reporting of Observational studies in Epidemiology(STROBE) cross-sectional reporting guidelines were used.
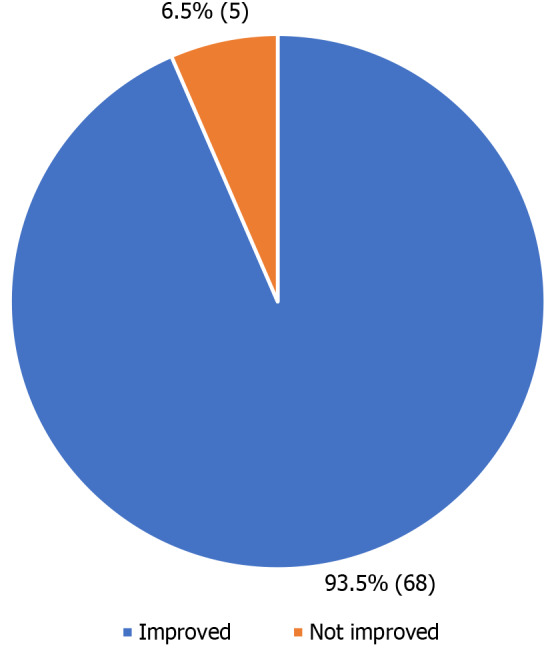
Results: Seventy-three patients had the InterStim implanted. The mean age was 63.29 ± 12.2 years. Fifty-seven (78.1%) patients were females and forty-two (57.5%) patients had diabetes. In addition to incontinence, overlapping symptoms included diarrhea (23.3%), fecal urgency (58.9%), and urinary incontinence (28.8%). Fifteen (20.5%) patients underwent Peripheral Nerve Evaluation before proceeding to definite implant placement. Thirty-two (43.8%) patients underwent rechargeable InterStim placement. Three (4.1%) patients needed removal of the implant. Migration of the external lead connection was observed in 7 (9.6%) patients after the stage I procedure. The explanation for one patient was due to infection. Seven (9.6%) patients had other complications like nerve pain, hematoma, infection, lead fracture, and bleeding. The mean follow-up was 6.62 ± 3.5 mo. Sixty-eight (93.2%) patients reported significant improvement of symptoms on follow-up evaluation.
Conclusion: This study shows promising results with significant symptom improvement, good efficacy and good patient outcomes with low complication rates while using MRI compatible InterStim for FI. Further long-term follow-up and future studies with a larger patient population is recommended.
Keywords: Fecal incontinence; InterStim; Magnetic resonance imaging; Sacral nerve stimulation; Sacral neuromodulation.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: No conflict of interest noted for any authors at the time of the study. This study was presented at the American Society of Colon and Rectal Surgeons Conference held in Tampa, Florida in 2022 and was published as an abstract. This study was also presented at the Fecal Incontinence and Obstructed Defecation Conference in 2022 which was held in Rome, Italy.
Figures
References
-
- Whitehead WE, Wald A, Norton NJ. Treatment options for fecal incontinence. Dis Colon Rectum. 2001;44:131–42; discussion 142. - PubMed
-
- Hughes BT, Chepyala P, Hendon S, Crowell MD, Olden KW. Fecal incontinence in an inpatient population: a not uncommon finding. Dig Dis Sci. 2009;54:2215–2219. - PubMed
-
- Nelson RL. Epidemiology of fecal incontinence. Gastroenterology. 2004;126:S3–S7. - PubMed
LinkOut - more resources
Full Text Sources
