

Latino-White Disparities in Identification and Control of Elevated Blood Pressure Among Adults With Hypertension
- PMID: 38456400
- PMCID: PMC11010015
- DOI: 10.1161/JAHA.123.033151
Latino-White Disparities in Identification and Control of Elevated Blood Pressure Among Adults With Hypertension
Abstract
Background: Studies analyzing blood pressure (BP) management using the hypertension control cascade have consistently shown disparities in hypertension awareness, treatment, and BP control between Latino patients and non-Latino White patients. We analyze this cascade using electronic health record data from a multistate network of community health centers.
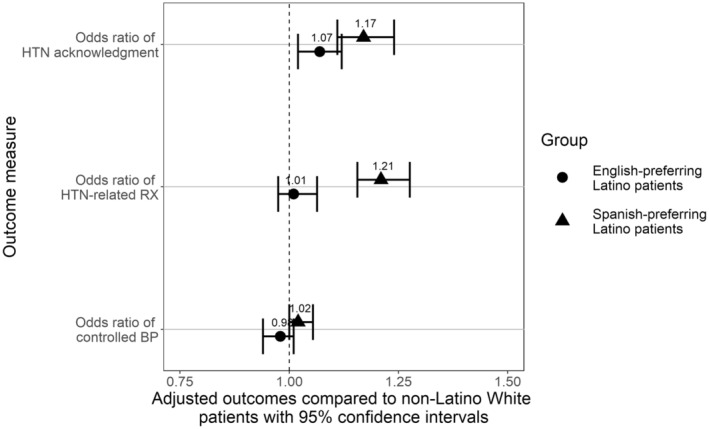
Methods and results: Data from 790 clinics in 23 US states from 2012 to 2020, including 1 270 174 patients, were analyzed to compare BP documentation in the electronic health record, clinician acknowledgment (diagnosis or treatment) of incident hypertension (BP ≥140/90), medication prescription, and BP control between non-Latino White patients, English-preferring Latino patients, and Spanish-preferring Latino patients, adjusted for patient-level covariates, and clustered on patients' primary clinics. Among the 429 182 patients with elevated BP (≥140/90) during ambulatory visits from 2012 to 2020, we found that clinician acknowledgment of hypertension was more likely in Spanish-preferring and English-preferring Latino patients versus non-Latino White patients (adjusted odds ratio [aOR], 1.17 [95% CI, 1.11-1.24]; aOR, 1.07 [95% CI, 1.02-1.12], respectively). In addition, Spanish-preferring Latino patients were more likely to receive a medication versus non-Latino White patients (aOR, 1.21 [95% CI, 1.16-1.28]). Among those receiving medication, Latino patients were as likely as non-Latino White patients to have their BP controlled (<140/90).
Conclusions: In a large retrospective study of community health center patients with incident hypertension, the expected disparities in hypertension management between Spanish-preferring Latino, English-preferring Latino, and non-Latino White patients were not identified. These findings add to the hypertension control cascade by examining robust electronic health record data from community health centers and may provide clues to reducing disparities in hypertension management.
Keywords: blood pressure; community health centers; disparities; hypertension control cascade.
Figures
Similar articles
-
Asthma Care Quality, Language, and Ethnicity in a Multi-State Network of Low-Income Children.J Am Board Fam Med. 2020 Sep-Oct;33(5):707-715. doi: 10.3122/jabfm.2020.05.190468. J Am Board Fam Med. 2020. PMID: 32989065 Free PMC article.
-
Latino-white disparities in ICD-coded asthma diagnosis among US children.J Asthma. 2022 Mar;59(3):514-522. doi: 10.1080/02770903.2020.1861628. Epub 2020 Dec 18. J Asthma. 2022. PMID: 33337260 Free PMC article.
-
Influenza and pneumococcal vaccination delivery in older Hispanic populations in the United States.J Am Geriatr Soc. 2022 Mar;70(3):854-861. doi: 10.1111/jgs.17589. Epub 2021 Dec 2. J Am Geriatr Soc. 2022. PMID: 34854478 Free PMC article.
-
Disparities in Colorectal Cancer Screening in Latinos and Non-Hispanic Whites.Am J Prev Med. 2022 Feb;62(2):203-210. doi: 10.1016/j.amepre.2021.07.009. Epub 2021 Oct 11. Am J Prev Med. 2022. PMID: 34649735 Free PMC article.
-
Disparities in COVID-19 Monoclonal Antibody Delivery: a Retrospective Cohort Study.J Gen Intern Med. 2022 Aug;37(10):2505-2513. doi: 10.1007/s11606-022-07603-4. Epub 2022 Apr 25. J Gen Intern Med. 2022. PMID: 35469360 Free PMC article. Review.
References
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Himmelfarb CD, DePalma SM, Gidding S, Jamerson KA, Jones DW, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:e140–e144. doi: 10.1161/HYP.0000000000000065 - DOI - PubMed
-
- Bundy JD, Li C, Stuchlik P, Bu X, Kelly TN, Mills KT, He H, Chen J, Whelton PK, He J. Systolic blood pressure reduction and risk of cardiovascular disease and mortality: a systematic review and network meta‐analysis. JAMA Cardiol. 2017;2:775–781. doi: 10.1001/jamacardio.2017.1421 - DOI - PMC - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective studies collaboration . Age‐specific relevance of usual blood pressure to vascular mortality: a meta‐analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. doi: 10.1016/s0140-6736(02)11911-8 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
