

Phase 3 Safety and Immunogenicity Study of a Three-dose Series of Twenty-valent Pneumococcal Conjugate Vaccine in Healthy Infants and Toddlers
- PMID: 38456705
- PMCID: PMC11090518
- DOI: 10.1097/INF.0000000000004300
Phase 3 Safety and Immunogenicity Study of a Three-dose Series of Twenty-valent Pneumococcal Conjugate Vaccine in Healthy Infants and Toddlers
Abstract
Background: Global pediatric immunization programs with pneumococcal conjugate vaccines (PCVs) have reduced vaccine-type pneumococcal disease, but a substantial disease burden of non-PCV serotypes remains.
Methods: This phase 3, randomized (1:1), double-blind study evaluated safety and immunogenicity of 20-valent PCV (PCV20) relative to 13-valent PCV (PCV13) in healthy infants. Participants received 2 infant doses and a toddler dose of PCV20 or PCV13, with diphtheria-tetanus-acellular pertussis combination vaccine at all doses and measles, mumps, rubella and varicella vaccines at the toddler dose. Primary pneumococcal immunogenicity objectives were to demonstrate noninferiority (NI) of PCV20 to PCV13 for immunoglobulin G geometric mean concentrations after infant and toddler doses and percentages of participants with predefined serotype-specific immunoglobulin G concentrations after infant doses. Safety endpoints included local reactions, systemic events and adverse events.
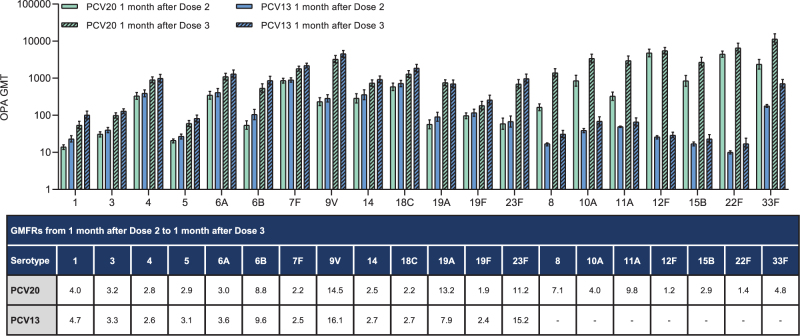
Results: Overall, 1204 participants were vaccinated (PCV20, n = 601; PCV13, n = 603). One month after the toddler dose, 19/20 serotypes met NI for immunoglobulin G geometric mean concentrations; serotype 6B narrowly missed NI [PCV20/PCV13 geometric mean ratio: 0.57 (2-sided 95% confidence interval: 0.48-0.67); NI criterion: lower 2-sided 95% confidence interval >0.5]. Sixteen/twenty serotypes met NI for ≥1 primary objective after 2 infant doses. PCV20 induced robust opsonophagocytic activity, and boosting responses were observed for all vaccine serotypes, including those missing statistical NI. The safety/tolerability profile of PCV20 was like that of PCV13.
Conclusions: PCV20 3-dose series in infants was safe and elicited robust immune responses. Based on these results and PCV13 experience, PCV20 3-dose series is expected to be protective for all 20 vaccine serotypes. NCT04546425.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Figures



References
-
- O’Brien KL, Wolfson LJ, Watt JP, et al. ; Hib and Pneumococcal Global Burden of Disease Study Team. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet. 2009;374:893–902. - PubMed
-
- Huang SS, Johnson KM, Ray GT, et al. . Healthcare utilization and cost of pneumococcal disease in the United States. Vaccine. 2011;29:3398–3412. - PubMed
-
- GBD 2016 Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Infect Dis. 2018;18:1191–1210. - PMC - PubMed
-
- Nuorti JP, Whitney CG; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children—use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59:1–18. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
