

The effect of an endovascular Heaney maneuver to achieve total hepatic isolation on survival, hemodynamic stability, retrohepatic bleeding, and collateral flow in a porcine model
- PMID: 38456908
- PMCID: PMC11458705
- DOI: 10.1007/s00068-024-02482-2
The effect of an endovascular Heaney maneuver to achieve total hepatic isolation on survival, hemodynamic stability, retrohepatic bleeding, and collateral flow in a porcine model
Abstract
Purpose: Combining resuscitative endovascular balloon occlusion of the aorta (REBOA) and the inferior vena cava (REBOVC) with open surgery is a new hybrid approach for treating retrohepatic vena caval injuries. We compared endovascular total hepatic isolation with supraceliac REBOA ± suprahepatic REBOVC and no occlusion in experimental retrohepatic vena cava bleeding regarding survival, bleeding volume, hemodynamic stability, and arterial collateral blood flow.
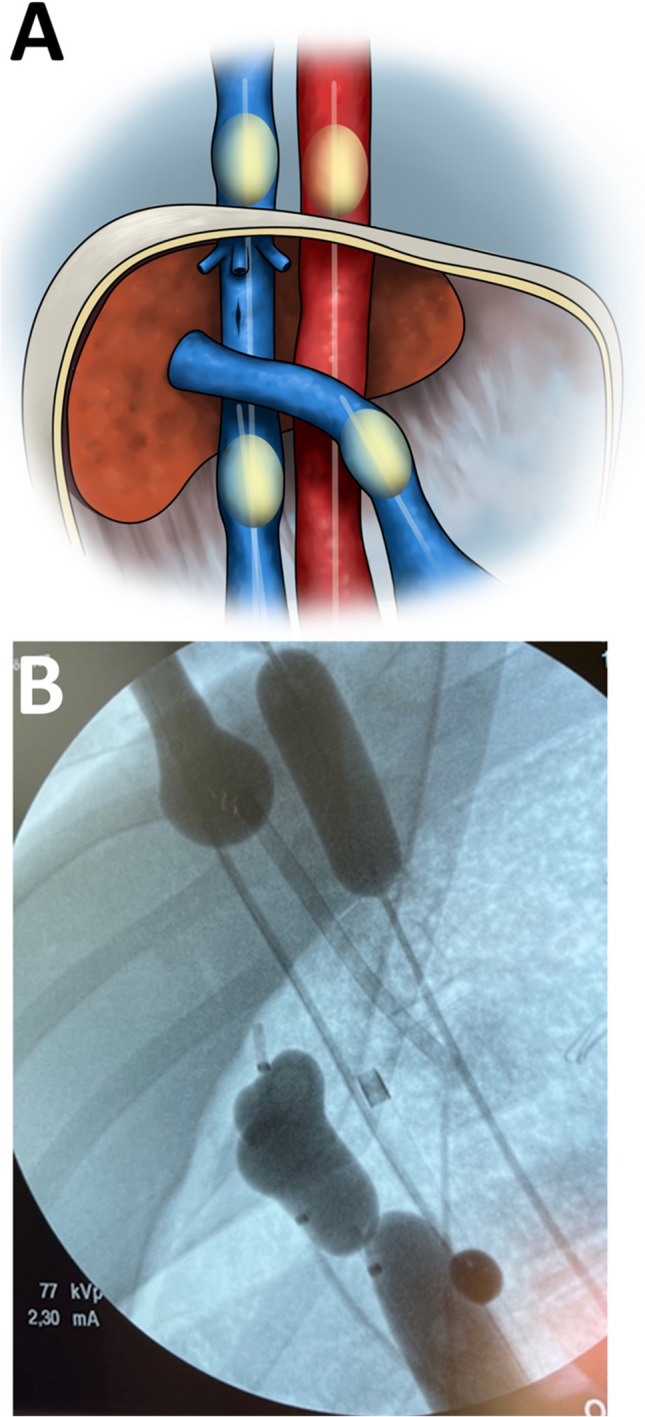
Methods: Twenty-five anesthetized pigs (n = 6-7/group) were randomized to REBOA; REBOA + REBOVC; REBOA + infra and suprahepatic REBOVC + portal vein occlusion (endovascular Heaney maneuver, four-balloon-occlusion, 4BO) or no occlusion. After balloon inflation, free bleeding was initiated from an open sheath in the retrohepatic vena cava. Bleeding volume, right internal thoracic artery (RITA) blood flow, hemodynamics, and arterial blood variables were measured until death or up to 90 min.
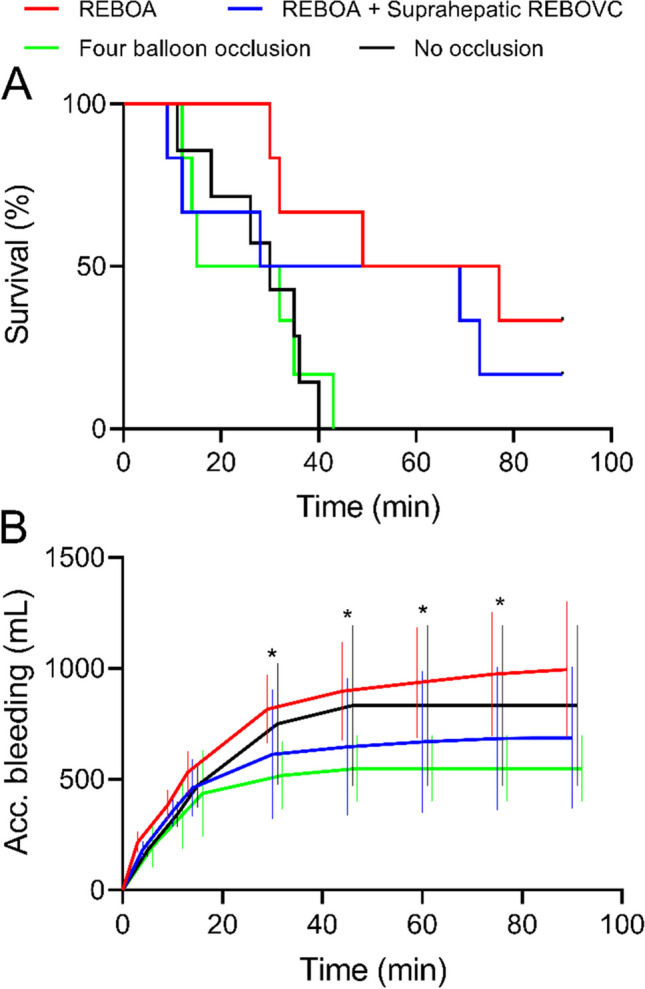
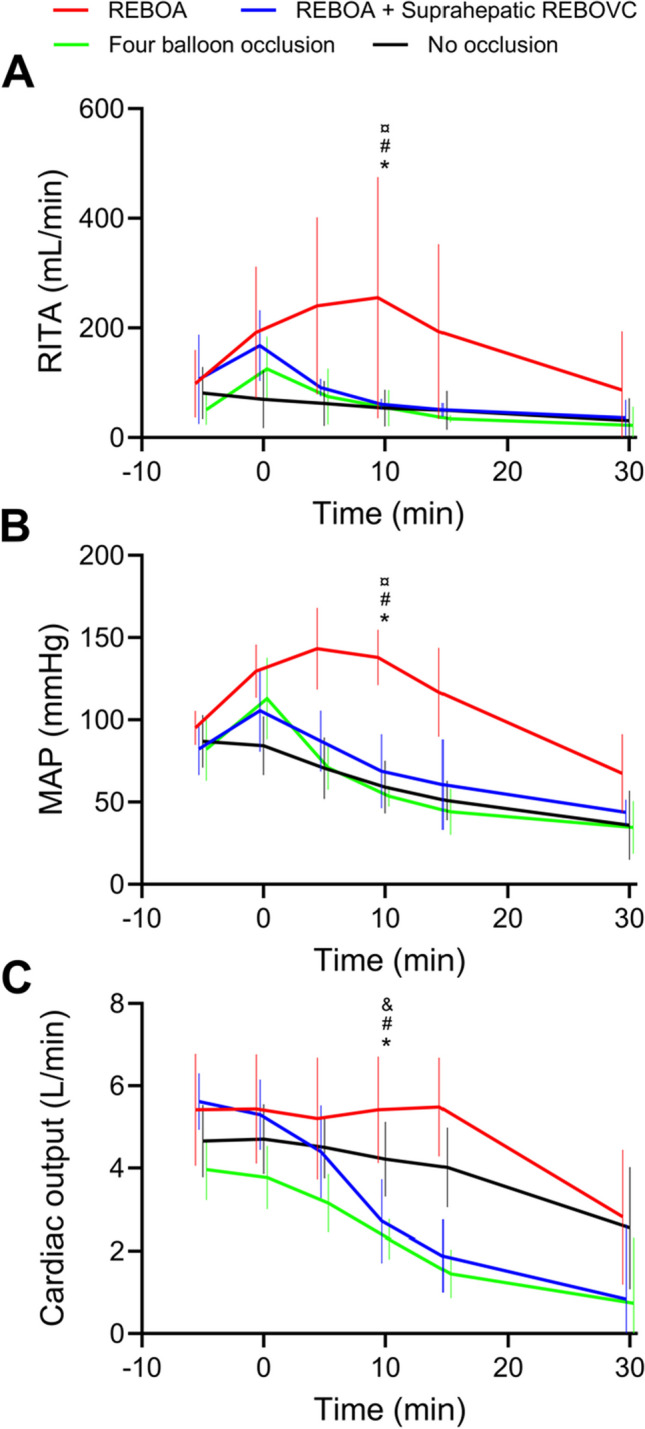
Results: The REBOA group had a longer median survival time (63 min) compared with the 4BO (24 min, P = 0.02) and no occlusion (30 min, P = 0.02) groups, not versus the REBOA + REBOVC group (49 min, P > 0.05). The first 15 min accumulated bleeding was comparable in all groups (P > 0.05); Thereafter, bleeding volume was higher in the REBOA group versus the 4BO group (P < 0.05), not versus the other groups. RITA blood flow and MAP were higher in the REBOA group versus the other groups after 10 min of bleeding (P < 0.05).
Conclusions: Endovascular Heaney maneuver was not beneficial for survival or hemodynamic stability in this porcine model, whereas supraceliac REBOA was. Anatomical differences in thoracoabdominal collaterals between pigs and humans must be considered when interpreting these results.
Keywords: REBOA; REBOVC; Retrohepatic inferior vena cava; Trauma.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
M.B. Wikström, A. Stene-Hurtsén, J. Åström, T.M. Hörer and K.F. Nilsson declare that they have no conflict of interests.
Figures

References
-
- Stonko DP, et al. Contemporary management and outcomes of injuries to the inferior vena cava: a prospective multicenter trial from prospective observational vascular injury treatment. Am Surg. 2021; 31348211038556. 10.1177/00031348211038556. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
