

Obstructive Sleep Apnea: The Effect of Bariatric Surgery After Five Years-A Prospective Multicenter Trial
- PMID: 38457003
- PMCID: PMC11031458
- DOI: 10.1007/s11695-024-07124-5
Obstructive Sleep Apnea: The Effect of Bariatric Surgery After Five Years-A Prospective Multicenter Trial
Abstract
Background: The prevalence of obstructive sleep apnea (OSA) is high among the bariatric surgery candidates. Obesity is the most important individual risk factor for OSA. The aim of this study was to investigate the effect of a laparoscopic Roux-en-Y gastric bypass (LRYGB) on OSA 5 years after the surgery.
Patients and methods: In this prospective multicenter study, standard overnight cardiorespiratory recording was conducted to 150 patients at baseline prior to bariatric surgery. A total of 111 (73.3%) patients of those had OSA. Cardiorespiratory recordings at 5 years after surgery were available for 70 OSA patients. The changes in anthropometric and demographic measurements including age, weight, body mass index (BMI), and waist and neck circumference were evaluated. Also, a quality of life (QoL) questionnaire 15D administered in a baseline was controlled at 5-year follow-up visit.
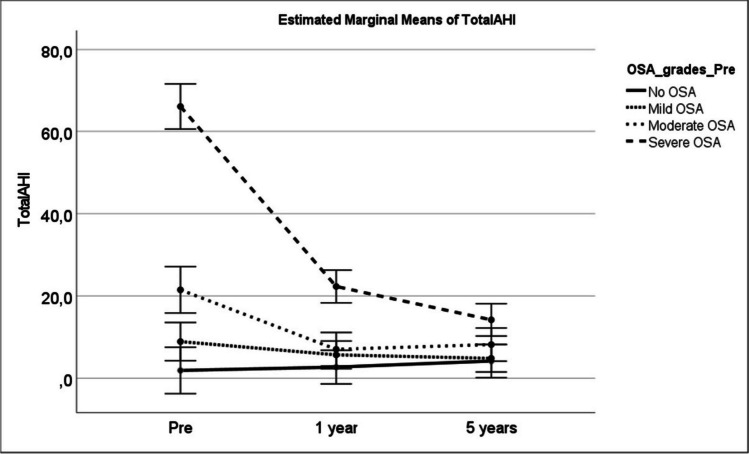
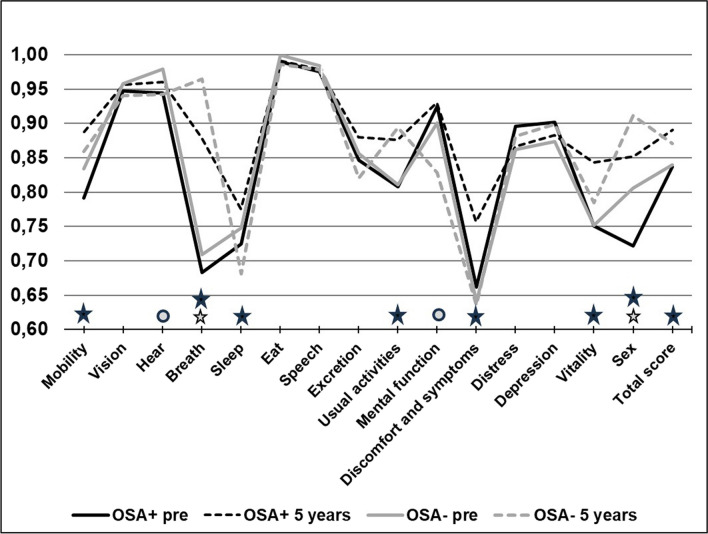
Results: At 5-year OSA was cured in 55% of patients, but moderate or severe OSA still persisted in 20% of patients after operation. Mean total AHI decreased from 27.8 events/h to 8.8 events/h (p < 0.001) at 5-year follow-up. A clinically significant difference in QoL was seen in mobility, breathing, sleeping, usual activities, discomfort and symptoms, vitality and sexual activity. The QoL total score improved more in OSA patient at 5-year follow-up.
Conclusions: LRYGB is an effective treatment of OSA in obese patients and the achieved beneficial outcomes are maintained at 5-year follow-up.
Keywords: Bariatric surgery; Effect of bariatric surgery; Metabolic surgery; OSA; Obesity surgery; Obstructive sleep apnea.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Obstructive sleep apnea: the effect of bariatric surgery after 12 months. A prospective multicenter trial.Sleep Med. 2017 Jul;35:85-90. doi: 10.1016/j.sleep.2016.12.017. Epub 2017 Jan 12. Sleep Med. 2017. PMID: 28549834 Clinical Trial.
-
Predictive Factors for Insufficient Weight Loss After Bariatric Surgery: Does Obstructive Sleep Apnea Influence Weight Loss?Obes Surg. 2016 May;26(5):1048-56. doi: 10.1007/s11695-015-1830-4. Obes Surg. 2016. PMID: 26220241
-
Prevalence of Obstructive Sleep Apnoea Among Patients Admitted for Bariatric Surgery. A Prospective Multicentre Trial.Obes Surg. 2016 Jul;26(7):1384-90. doi: 10.1007/s11695-015-1953-7. Obes Surg. 2016. PMID: 26559426
-
Bariatric surgery and obstructive sleep apnea: a systematic review and meta-analysis.Sleep Breath. 2023 Dec;27(6):2283-2294. doi: 10.1007/s11325-023-02840-1. Epub 2023 May 5. Sleep Breath. 2023. PMID: 37145243
-
Prevalence of obstructive sleep apnea in an Asian bariatric population: an underdiagnosed dilemma.Surg Obes Relat Dis. 2020 Jun;16(6):778-783. doi: 10.1016/j.soard.2020.02.003. Epub 2020 Feb 19. Surg Obes Relat Dis. 2020. PMID: 32199766 Review.
Cited by
-
Efficacy and Safety of Glucagon Like Peptide-1 Receptor Agonism Based Therapies in Obstructive Sleep Apnoea: A Systematic Review and Meta-Analysis.Indian J Endocrinol Metab. 2025 Jan-Feb;29(1):4-12. doi: 10.4103/ijem.ijem_365_24. Epub 2025 Feb 28. Indian J Endocrinol Metab. 2025. PMID: 40181850 Free PMC article. Review.
-
Outcomes and Safety of One Anastomosis Gastric Bypass (OAGB): A Three-Year Retrospective Study.Obes Surg. 2025 Aug 8. doi: 10.1007/s11695-025-08150-7. Online ahead of print. Obes Surg. 2025. PMID: 40779280 Review.
-
Sleep Quality and Bariatric Surgery-Can We Treat Sleep Disturbances and Insomnia in Patients with Obesity with Laparoscopic Sleeve Gastrectomy?J Clin Med. 2024 Aug 15;13(16):4820. doi: 10.3390/jcm13164820. J Clin Med. 2024. PMID: 39200961 Free PMC article.
-
New Insights of Cardiac Arrhythmias Associated with Sleep-Disordered Breathing: From Mechanisms to Clinical Implications-A Narrative Review.J Clin Med. 2025 Mar 12;14(6):1922. doi: 10.3390/jcm14061922. J Clin Med. 2025. PMID: 40142730 Free PMC article. Review.
-
Health outcomes and their association with weight regain after substantial weight loss in Sweden: a prospective cohort study.Lancet Reg Health Eur. 2025 Mar 13;52:101261. doi: 10.1016/j.lanepe.2025.101261. eCollection 2025 May. Lancet Reg Health Eur. 2025. PMID: 40166366 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
