

Activation of CGRP receptor-mediated signaling promotes tendon-bone healing
- PMID: 38457499
- PMCID: PMC10923525
- DOI: 10.1126/sciadv.adg7380
Activation of CGRP receptor-mediated signaling promotes tendon-bone healing
Abstract
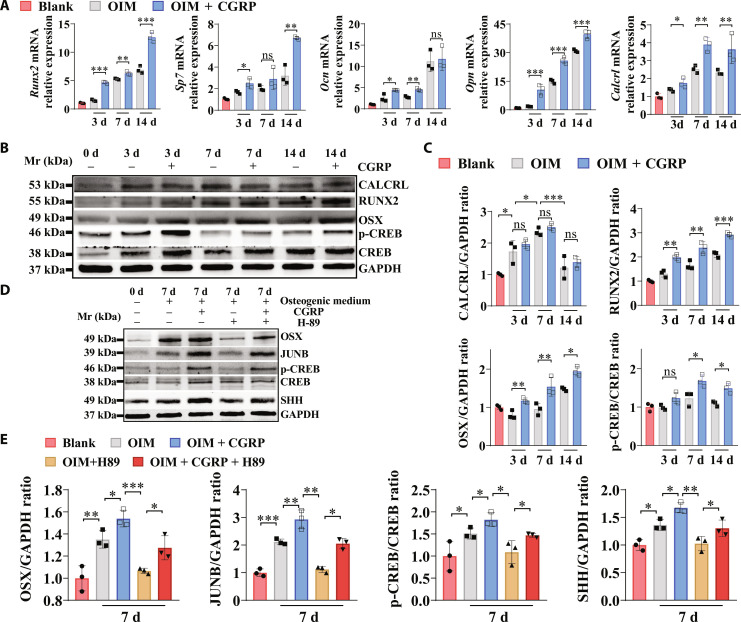
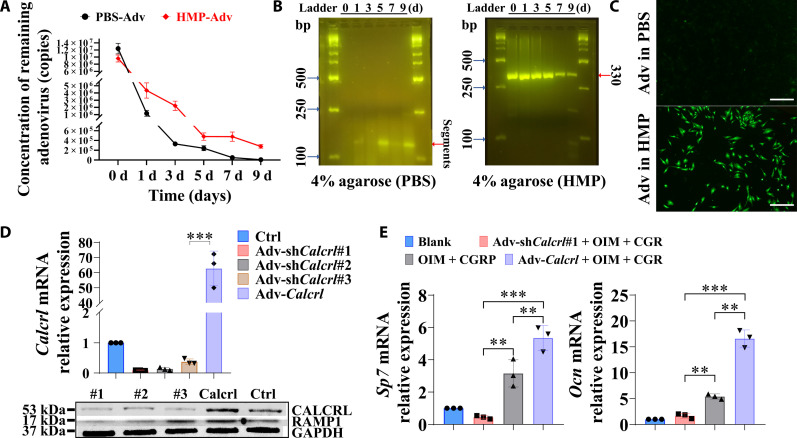
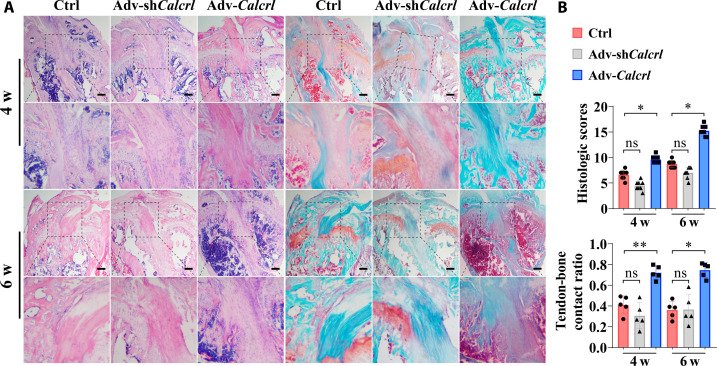
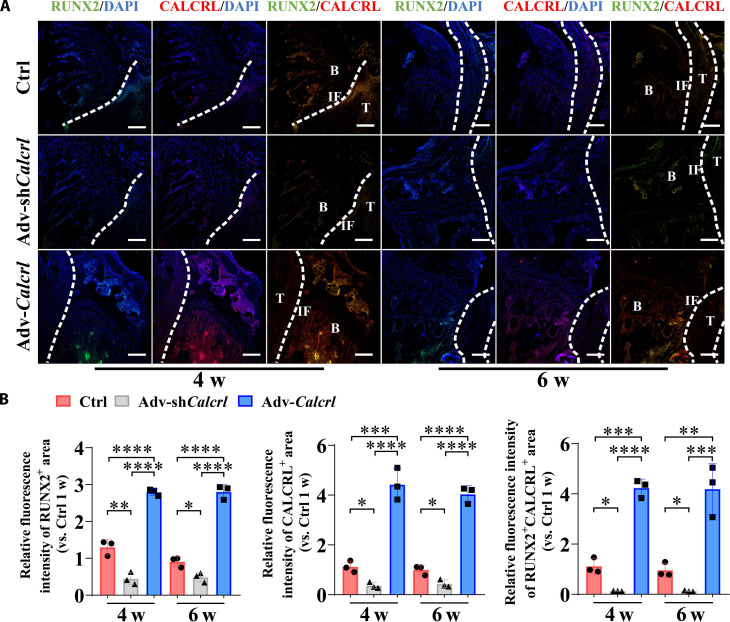
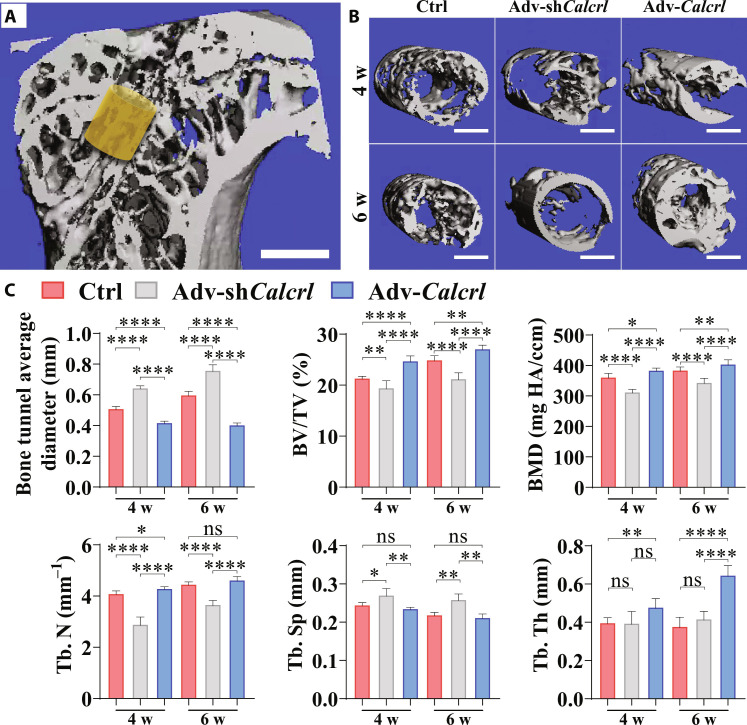
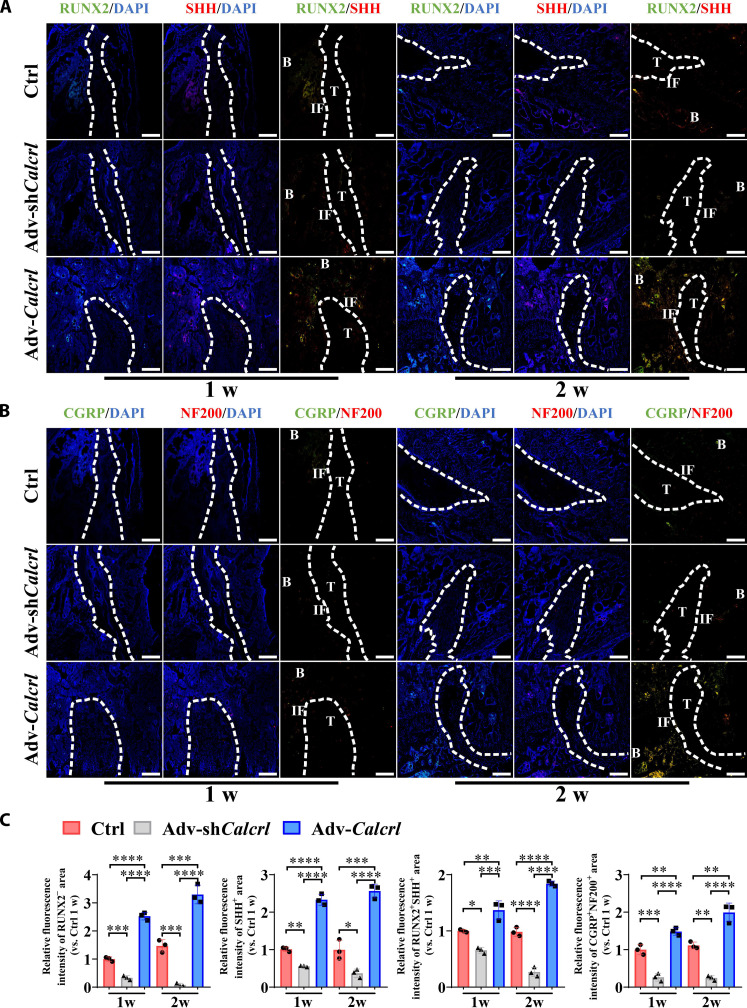
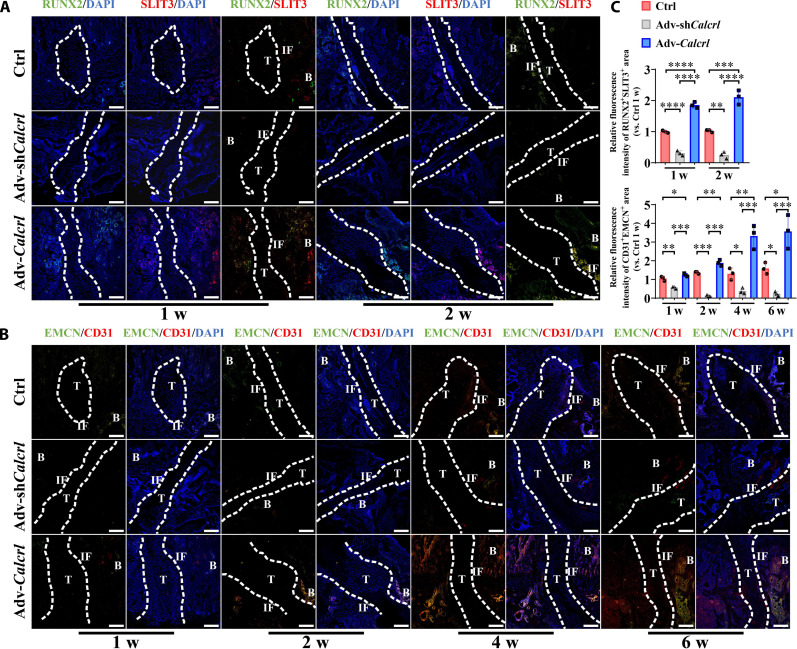
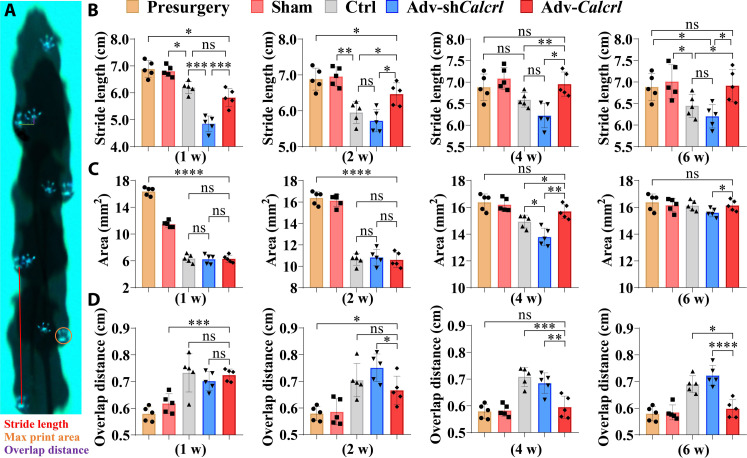
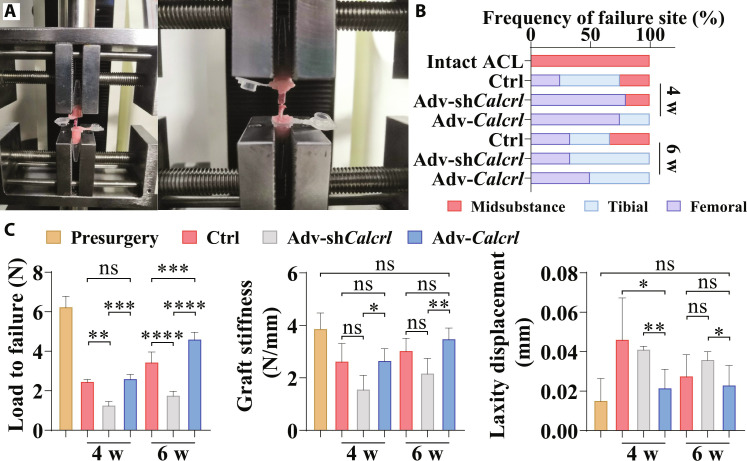
Calcitonin gene-related peptide (CGRP), an osteopromotive neurotransmitter with a short half-life, shows increase while calcitonin receptor-like (CALCRL) level is decreased at the early stage in bone fractures. Therefore, the activation of CALCRL-mediated signaling may be more critical to promote the tendon-bone healing. We found CGRP enhanced osteogenic differentiation of BMSCs through PKA/CREB/JUNB pathway, contributing to improved sonic hedgehog (SHH) expression, which was verified at the tendon-bone interface (TBI) in the mice with Calcrl overexpression. The osteoblast-derived SHH and slit guidance ligand 3 were reported to favor nerve regeneration and type H (CD31hiEMCNhi) vessel formation, respectively. Encouragingly, the activation or inactivation of CALCRL-mediated signaling significantly increased or decreased intensity of type H vessel and nerve fiber at the TBI, respectively. Simultaneously, improved gait characteristics and biomechanical performance were observed in the Calcrl overexpression group. Together, the gene therapy targeting CGRP receptor may be a therapeutic strategy in sports medicine.
Figures
References
-
- Sherman S. L., Calcei J., Ray T., Magnussen R. A., Musahl V., Kaeding C. C., Clatworthy M., Bergfeld J. A., Arnold M. P., ACL Study Group presents the global trends in ACL reconstruction: Biennial survey of the ACL Study Group. J. ISAKOS 6, 322–328 (2021). - PubMed
-
- Renstrom P. A., Eight clinical conundrums relating to anterior cruciate ligament (ACL) injury in sport: Recent evidence and a personal reflection. Br. J. Sports Med. 47, 367–372 (2013). - PubMed
-
- Crawford S. N., Waterman B. R., Lubowitz J. H., Long-term failure of anterior cruciate ligament reconstruction. Art Ther. 29, 1566–1571 (2013). - PubMed
-
- Rothrauff B. B., Jorge A., de Sa D., Kay J., Fu F. H., Musahl V., Anatomic ACL reconstruction reduces risk of post-traumatic osteoarthritis: A systematic review with minimum 10-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 28, 1072–1084 (2020). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
