

Treatment of unilateral cervical facet fractures without evidence of dislocation or subluxation: a narrative review and proposed treatment algorithm
- PMID: 38457922
- PMCID: PMC10958245
- DOI: 10.1530/EOR-23-0161
Treatment of unilateral cervical facet fractures without evidence of dislocation or subluxation: a narrative review and proposed treatment algorithm
Abstract
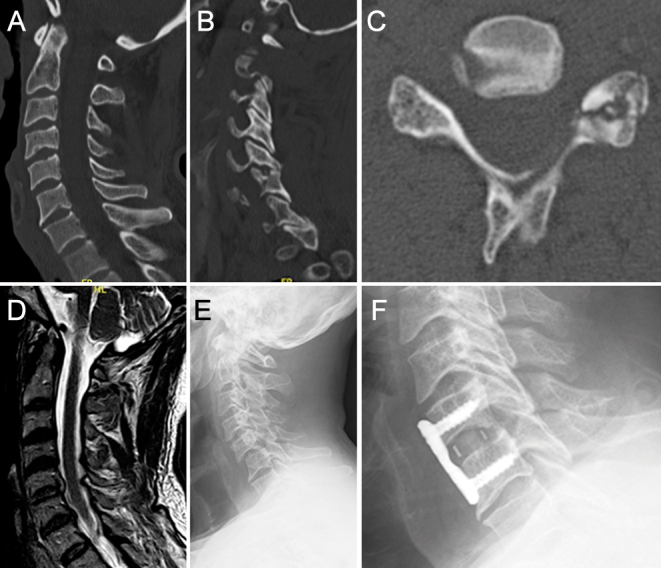
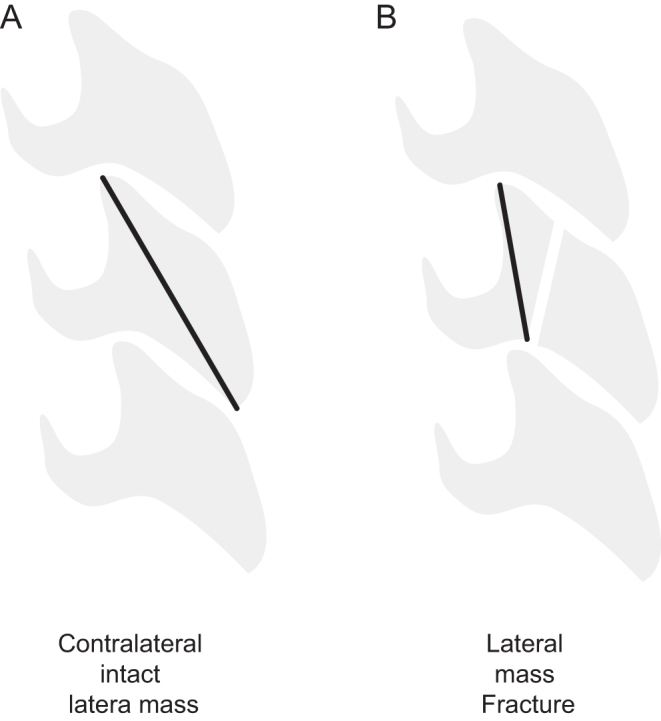
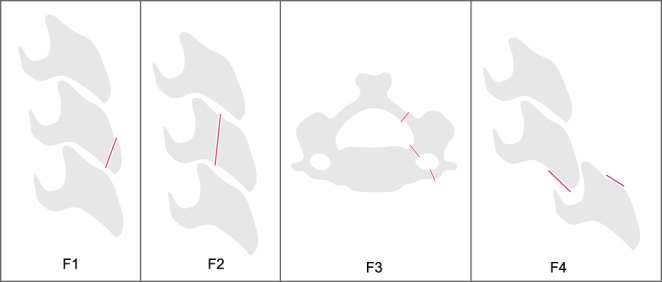
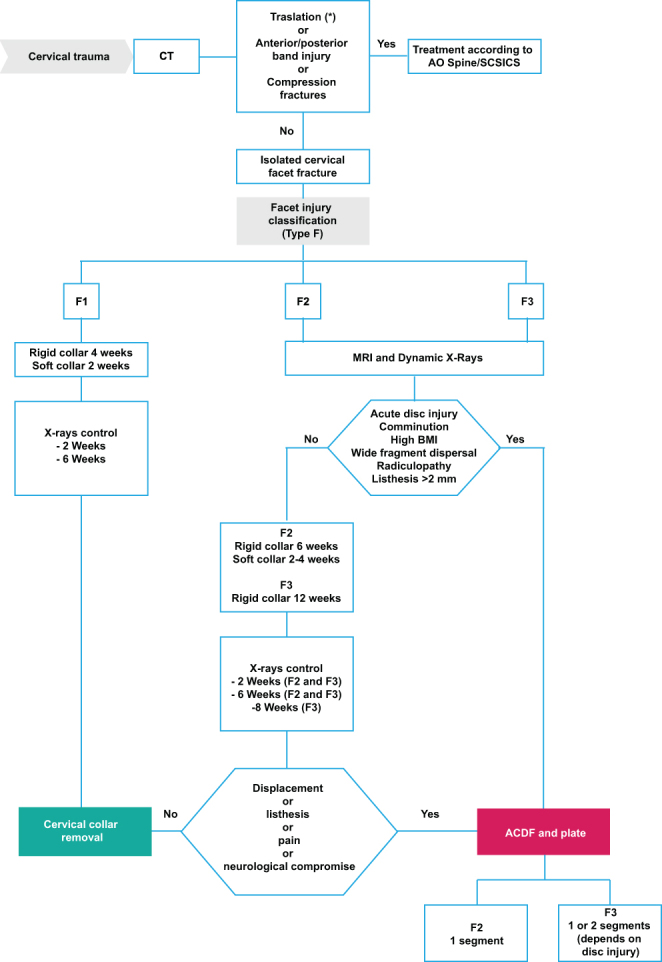
Isolated cervical spine facet fractures are often overlooked. The primary imaging modality for diagnosing these injuries is a computed tomography scan. Treatment of unilateral cervical facet fractures without evidence of dislocation or subluxation remains controversial. The available evidence regarding treatment options for these fractures is of low quality. Risk factors associated with the failure of nonoperative treatment are: comminution of the articular mass or facet joint, acute radiculopathy, high body mass index, listhesis exceeding 2 mm, fragmental diastasis, acute disc injury, and bilateral fractures or fractures that adversely affect 40% of the intact lateral mass height or have an absolute height of 1 cm.
Keywords: Spine; cervical facet fracture; isolated; non-displaced; trauma.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of this review.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
