

Paclitaxel-Coated Balloon vs Uncoated Balloon for Coronary In-Stent Restenosis: The AGENT IDE Randomized Clinical Trial
- PMID: 38460161
- PMCID: PMC10924708
- DOI: 10.1001/jama.2024.1361
Paclitaxel-Coated Balloon vs Uncoated Balloon for Coronary In-Stent Restenosis: The AGENT IDE Randomized Clinical Trial
Abstract
Importance: Drug-coated balloons offer a potentially beneficial treatment strategy for the management of coronary in-stent restenosis. However, none have been previously evaluated or approved for use in coronary circulation in the United States.
Objective: To evaluate whether a paclitaxel-coated balloon is superior to an uncoated balloon in patients with in-stent restenosis undergoing percutaneous coronary intervention.
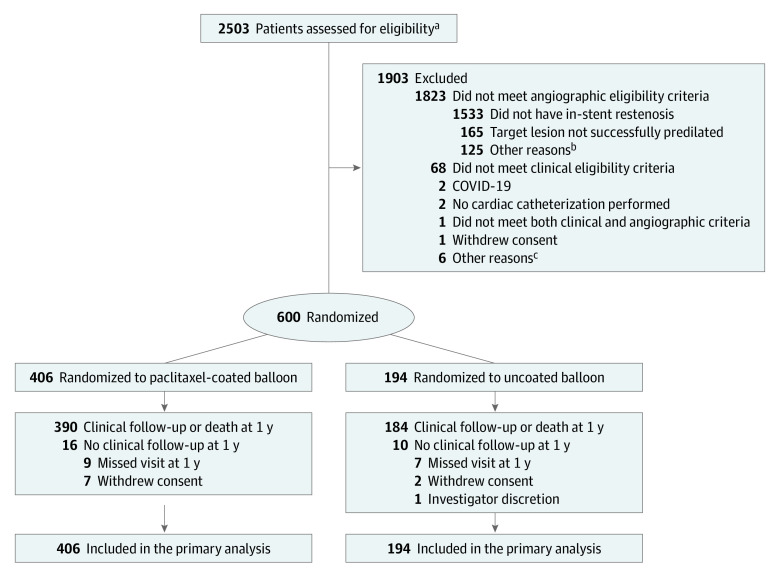
Design, setting, and participants: AGENT IDE, a multicenter randomized clinical trial, enrolled 600 patients with in-stent restenosis (lesion length <26 mm and reference vessel diameter >2.0 mm to ≤4.0 mm) at 40 centers across the United States between May 2021 and August 2022. One-year clinical follow-up was completed on October 2, 2023.
Interventions: Participants were randomized in a 2:1 allocation to undergo treatment with a paclitaxel-coated (n = 406) or an uncoated (n = 194) balloon.
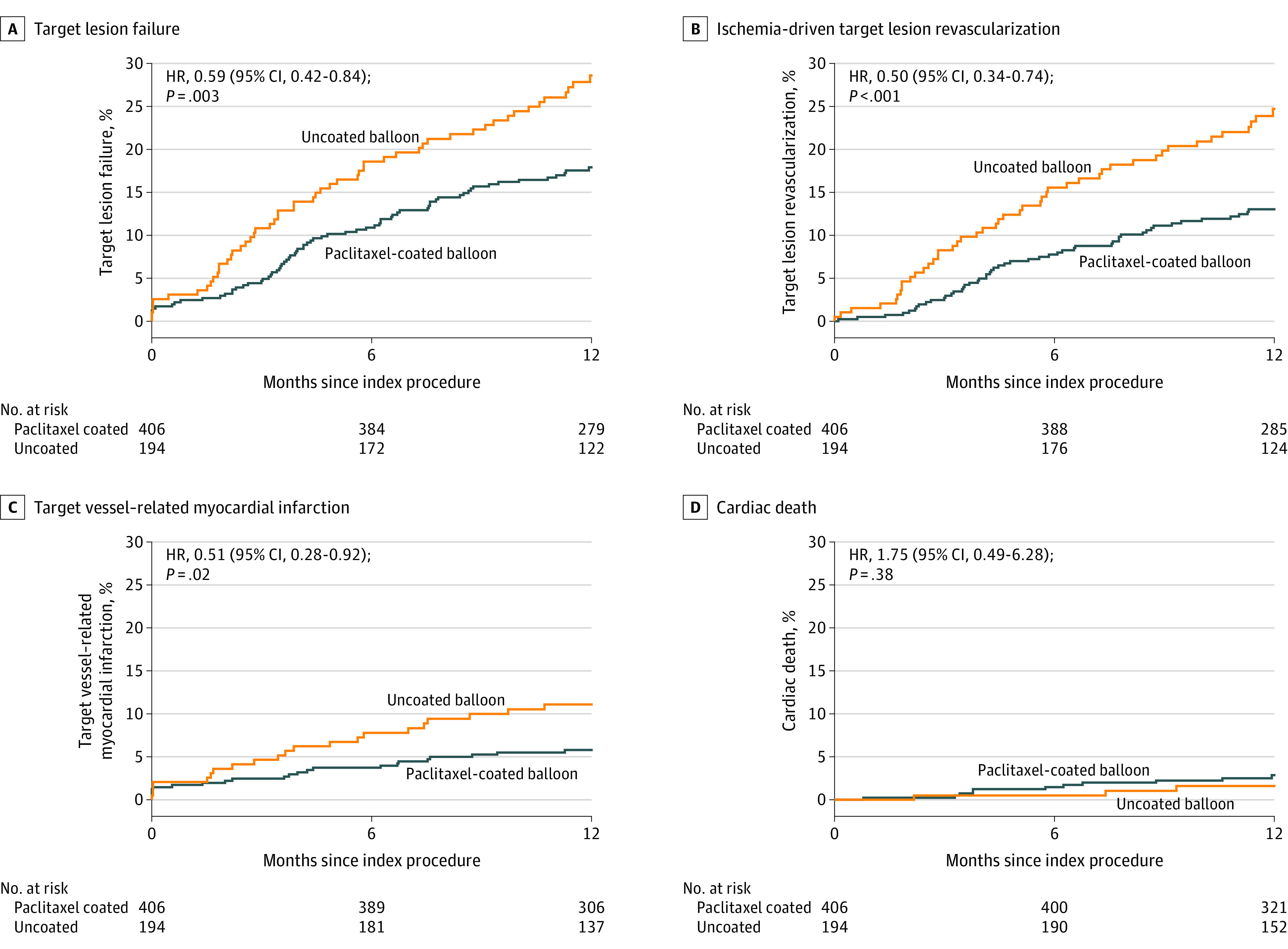
Main outcomes and measures: The primary end point of 1-year target lesion failure-defined as the composite of ischemia-driven target lesion revascularization, target vessel-related myocardial infarction, or cardiac death-was tested for superiority.
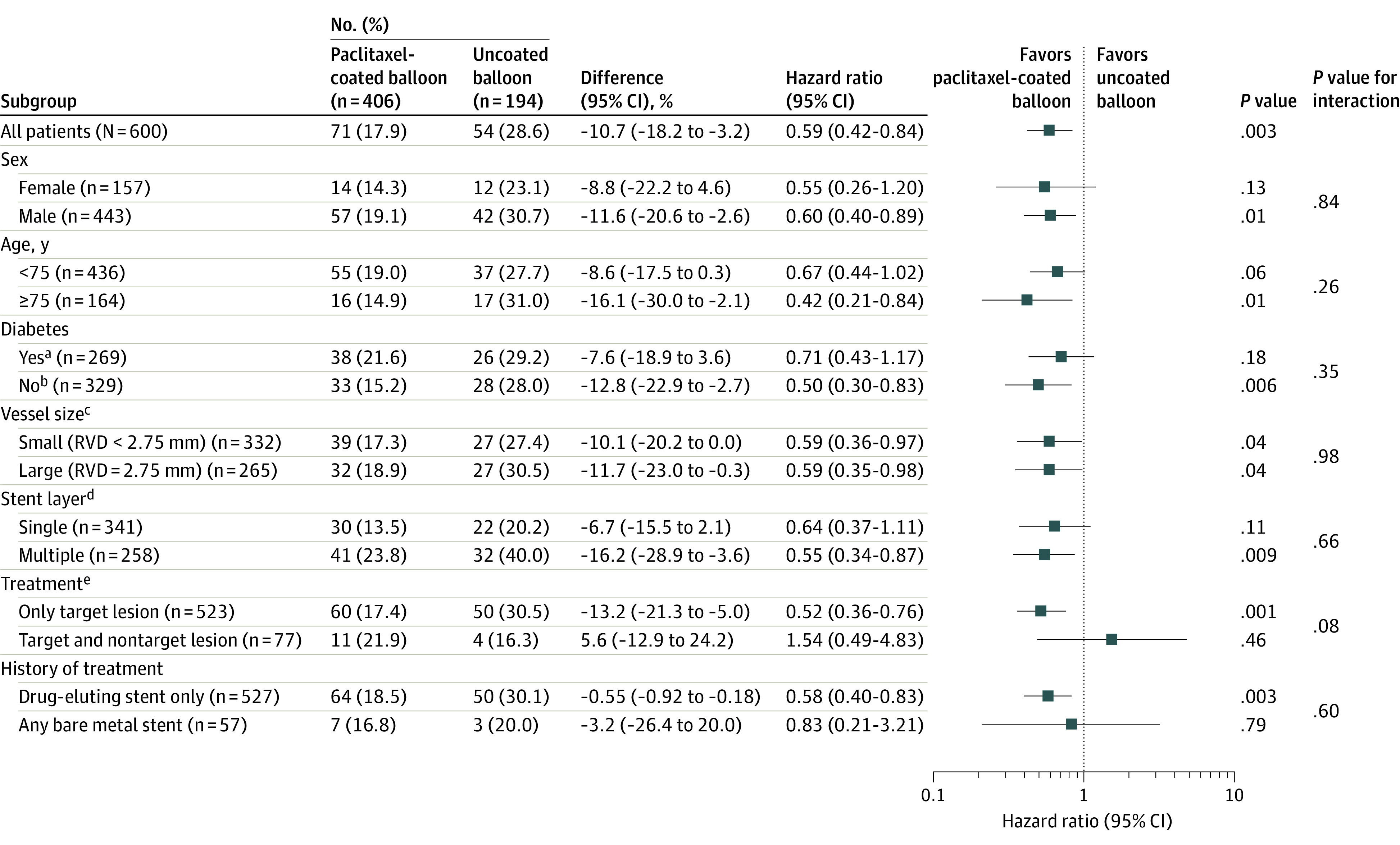
Results: Among 600 randomized patients (mean age, 68 years; 157 females [26.2%]; 42 Black [7%], 35 Hispanic [6%] individuals), 574 (95.7%) completed 1-year follow-up. The primary end point at 1 year occurred in 17.9% in the paclitaxel-coated balloon group vs 28.6% in the uncoated balloon group, meeting the criteria for superiority (hazard ratio [HR], 0.59 [95% CI, 0.42-0.84]; 2-sided P = .003). Target lesion revascularization (13.0% vs 24.7%; HR, 0.50 [95% CI, 0.34-0.74]; P = .001) and target vessel-related myocardial infarction (5.8% vs 11.1%; HR, 0.51 [95% CI, 0.28-0.92]; P = .02) occurred less frequently among patients treated with paclitaxel-coated balloon. The rate of cardiac death was 2.9% vs 1.6% (HR, 1.75 [95% CI, 0.49-6.28]; P = .38) in the coated vs uncoated balloon groups, respectively.
Conclusions and relevance: Among patients undergoing coronary angioplasty for in-stent restenosis, a paclitaxel-coated balloon was superior to an uncoated balloon with respect to the composite end point of target lesion failure. Paclitaxel-coated balloons are an effective treatment option for patients with coronary in-stent restenosis.
Trial registration: ClinicalTrials.gov Identifier: NCT04647253.
Conflict of interest statement
Figures
Comment in
-
Drug-Coated Balloons for In-Stent Restenosis-Finally Leaving Nothing Behind for US Patients.JAMA. 2024 Mar 26;331(12):1011-1012. doi: 10.1001/jama.2024.0813. JAMA. 2024. PMID: 38460158 No abstract available.
References
-
- Byrne RA, Neumann FJ, Mehilli J, et al. ; ISAR-DESIRE 3 investigators . Paclitaxel-eluting balloons, paclitaxel-eluting stents, and balloon angioplasty in patients with restenosis after implantation of a drug-eluting stent (ISAR-DESIRE 3): a randomised, open-label trial. Lancet. 2013;381(9865):461-467. doi: 10.1016/S0140-6736(12)61964-3 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
