

Circulating tumor DNA for predicting recurrence in patients with operable breast cancer: a systematic review and meta-analysis
- PMID: 38460249
- PMCID: PMC10940943
- DOI: 10.1016/j.esmoop.2024.102390
Circulating tumor DNA for predicting recurrence in patients with operable breast cancer: a systematic review and meta-analysis
Abstract
Background: The incorporation of circulating tumor DNA (ctDNA) into the management of operable breast cancer (BC) has been hampered by the heterogeneous results from different studies. We aimed to assess the prognostic value of ctDNA in patients with operable (non metastatic) BC.
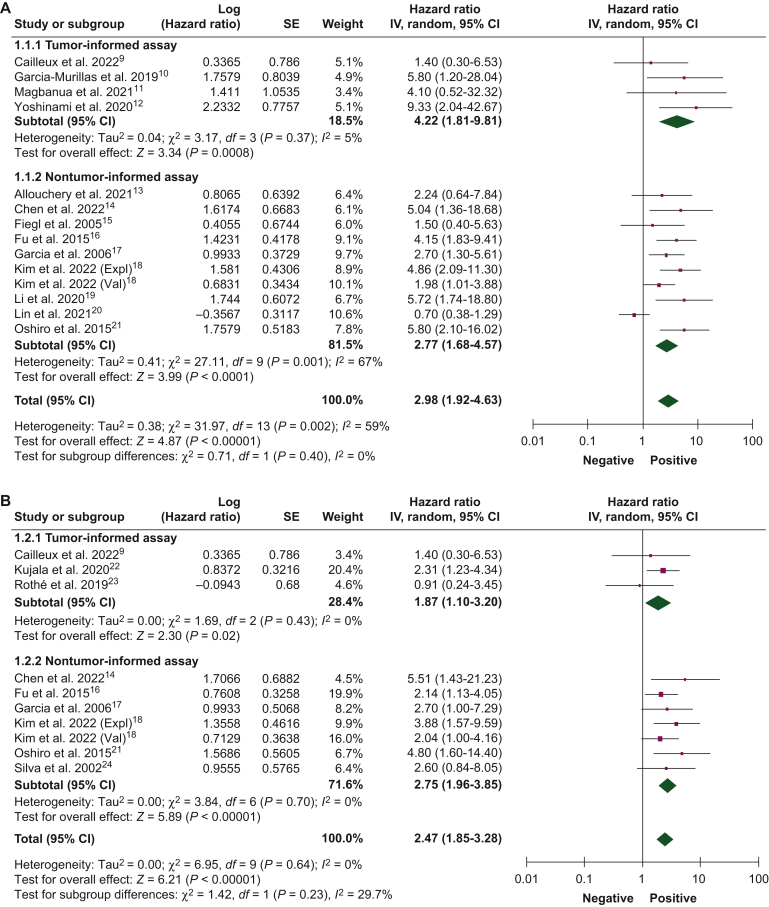
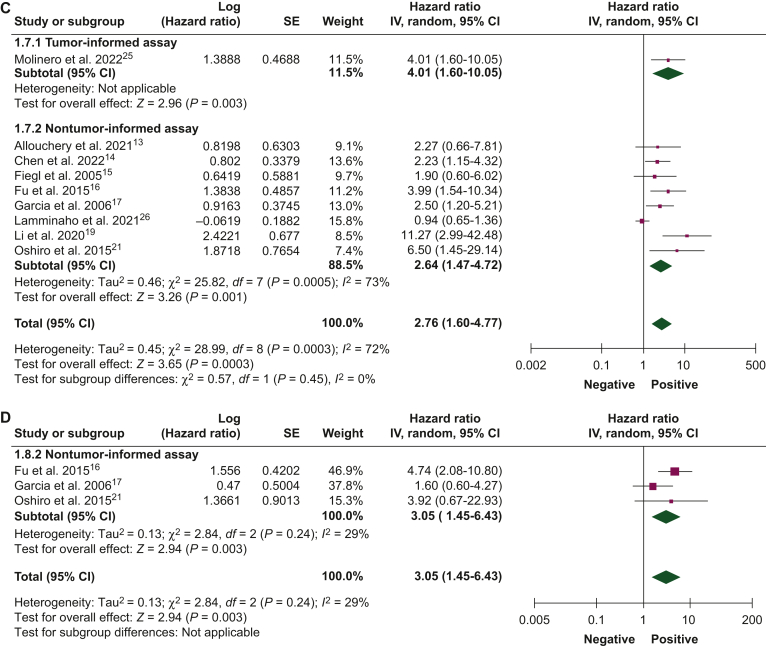
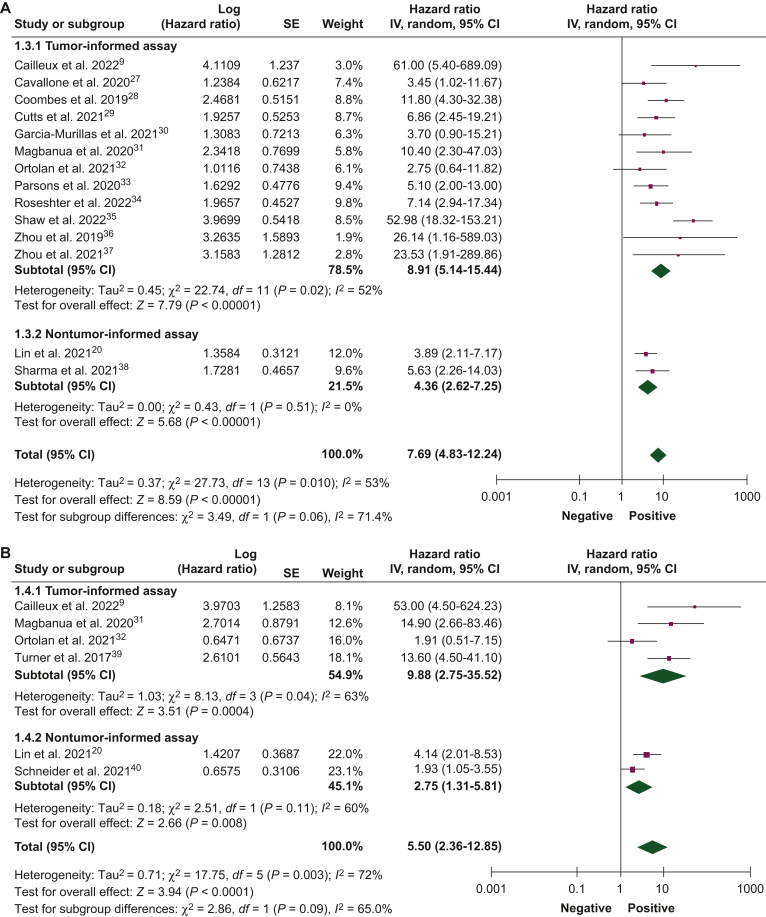
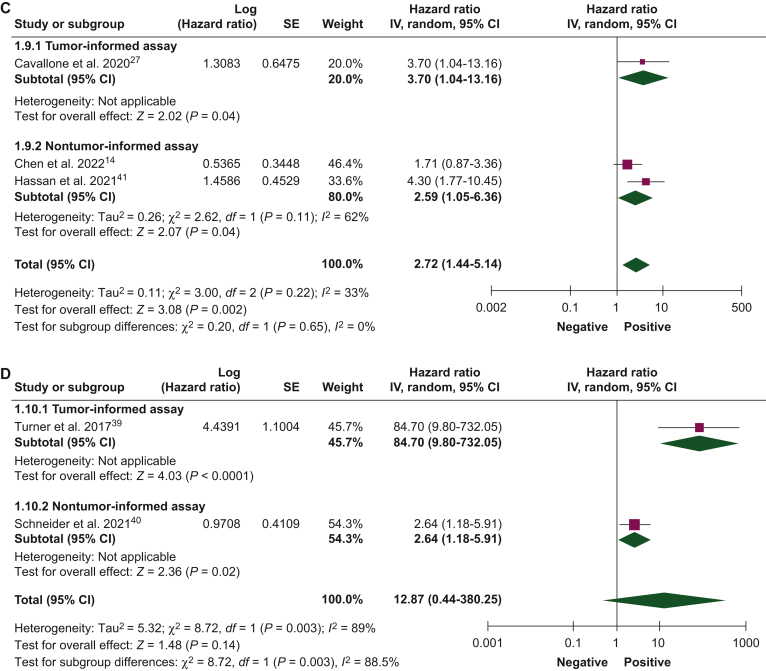
Materials and methods: A systematic search of databases (PubMed/Medline, Embase, and CENTRAL) and conference proceedings was conducted to identify studies reporting the association of ctDNA detection with disease-free survival (DFS) and overall survival (OS) in patients with stage I-III BC. Log-hazard ratios (HRs) were pooled at each timepoint of ctDNA assessment (baseline, after neoadjuvant therapy, and follow-up). ctDNA assays were classified as primary tumor-informed and non tumor-informed.
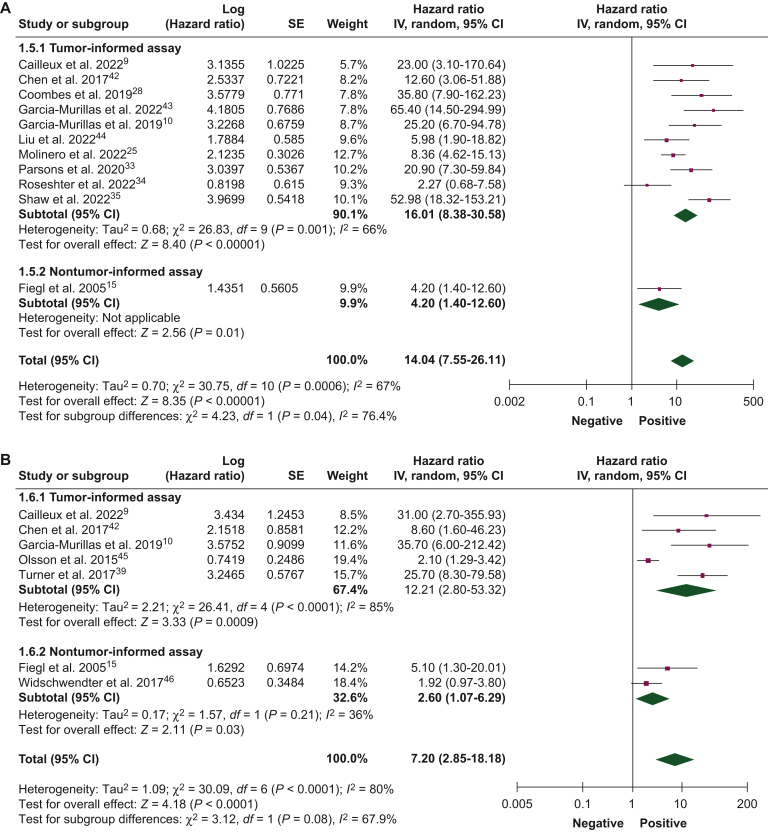
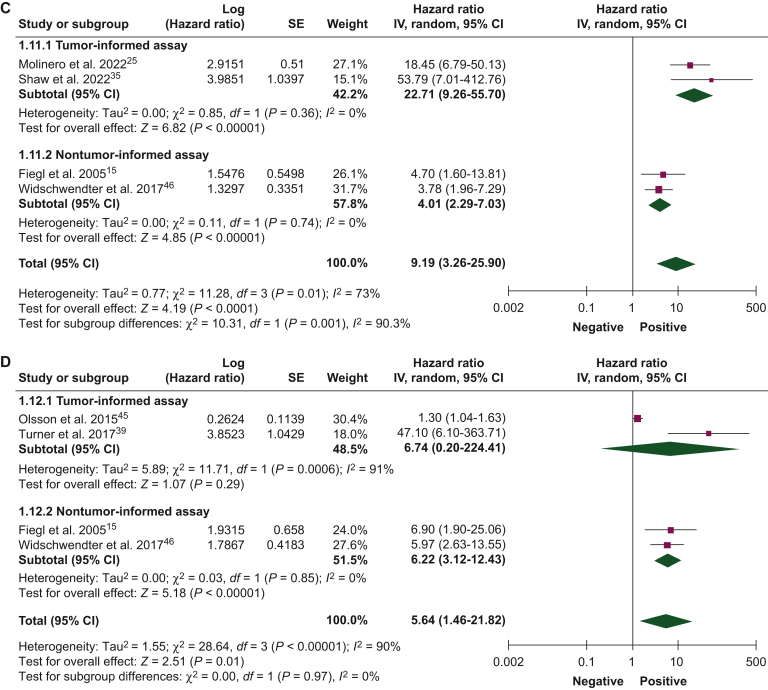
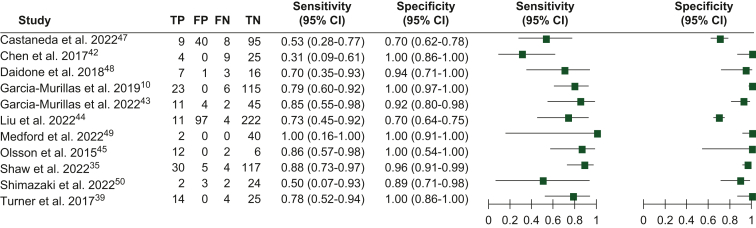
Results: Of the 3174 records identified, 57 studies including 5779 patients were eligible. In univariate analyses, ctDNA detection was associated with worse DFS at baseline [HR 2.98, 95% confidence interval (CI) 1.92-4.63], after neoadjuvant therapy (HR 7.69, 95% CI 4.83-12.24), and during follow-up (HR 14.04, 95% CI 7.55-26.11). Similarly, ctDNA detection at all timepoints was associated with worse OS (at baseline: HR 2.76, 95% CI 1.60-4.77; after neoadjuvant therapy: HR 2.72, 95% CI 1.44-5.14; and during follow-up: HR 9.19, 95% CI 3.26-25.90). Similar DFS and OS results were observed in multivariate analyses. Pooled HRs were numerically higher when ctDNA was detected at the end of neoadjuvant therapy or during follow-up and for primary tumor-informed assays. ctDNA detection sensitivity and specificity for BC recurrence ranged from 0.31 to 1.0 and 0.7 to 1.0, respectively. The mean lead time from ctDNA detection to overt recurrence was 10.81 months (range 0-58.9 months).
Conclusions: ctDNA detection was associated with worse DFS and OS in patients with operable BC, particularly when detected after treatment and using primary tumor-informed assays. ctDNA detection has a high specificity for anticipating BC relapse.
Keywords: breast neoplasms; circulating tumor DNA; disease-free survival; liquid biopsy; prognosis; sensitivity and specificity; tumor biomarker.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure GNM reports meeting/travel grants from AstraZeneca. EA reports consultancy fees/honoraria from Eli Lilly, Sandoz, and AstraZeneca; research grant to the institution from Gilead; meeting/travel grants from Novartis, Roche, Eli Lilly, Genetic, Istituto Gentili, Daiichi Sankyo, and AstraZeneca (all outside the submitted work). DMB reports full time employment at European Society for Medical Oncology since September 1, 2023; speaker’s engagement from Daiichi Sankyo/AstraZeneca; participation as medical research fellow in research studies with institutionally funded by Eli Lilly, Novartis, and F. Hoffmann-La Roche Ltd to Institut Jules Bordet; non-financial interest as member of the board of directors for Associaҫão de Investigaҫão e Ciudados de Suporte em Oncologia; non-remunerated prior leadership role as Portuguese Young Oncologists Committee Chair from Sociedade Portuguesa de Oncologia (all outside the submitted work). ALC reports leadership role at Eisai, Celgene, Lilly, Pfizer, Roche, Novartis, and MSD; intellectual property for MEDSIR; a consulting role for Lilly, Roche, Pfizer, Novartis, Pierre-Fabre, Exact Sciences, Seagen, and GSK; to be part of the speaker bureau for Lilly, AstraZeneca, and MSD; to receive research funding from Pfizer, Roche, Foundation Medicine, Exact Sciences, Pierre-Fabre, and Agendia; and travel compensation from Roche, Lilly, Novartis, Pfizer, and AstraZeneca. JC reports consulting/advisor role for Roche, Celgene, Cellestia, AstraZeneca, Seattle Genetics, Daiichi Sankyo, Erytech, Athenex, Polyphor, Lilly, Merck Sharp & Dohme, GSK, Leuko, Bioasis, Clovis Oncology, Boehringer Ingelheim, Ellipses, HiberCell, BioInvent, GEMoaB, Gilead, Menarini, Zymeworks, Reveal Genomics, Expres2ion Biotechnologies, Jazz Pharmaceuticals, and AbbVie; honoraria from Roche, Novartis, Celgene, Eisai, Pfizer, Samsung Bioepis, Lilly, Merck Sharp & Dohme, Daiichi Sankyo, AstraZeneca; research funding to the institution from Roche, Ariad pharmaceuticals, AstraZeneca, Baxalta GMBH/Servier Affaires, Bayer healthcare, Eisai, F. Hoffmann-La Roche, Guardant Health, Merck Sharp & Dohme, Pfizer, PIQUR Therapeutics, IQVIA, and Queen Mary University of London; stocks from MAJ3 Capital and Leuko (relative); travel, accommodation, and other expenses covered by Roche, Novartis, Eisai, Pfizer, Daiichi Sankyo, AstraZeneca, Gilead, and Merck Sharp & Dohme; patents ‘Pharmaceutical Combinations of A Pi3k Inhibitor And A Microtubule Destabilizing Agent’—Javier Cortés Castán, Alejandro Piris Giménez, Violeta Serra Elizalde, WO 2014/199294 A (issued) and ‘Her2 as a predictor of response to dual HER2 blockade in the absence of cytotoxic therapy’—Aleix Prat, Antonio Llombart, Javier Cortés, US 2019/ 0338368 A1 (licensed). MI reports honoraria from Novartis and Seattle Genetics; research support to the institution from Natera Inc, Inivata, Roche, and Pfizer; and travel grants from Roche and Gilead. GP reports being part of the advisory board/speaker bureau for Roche, Bayer, AstraZeneca, Novartis, Illumina, and ADS Biotech; and grants from Candriam and Thermo Fisher. EA reports honoraria and/or being part of the advisory board for Roche/GNE, Novartis, Seagen, Zodiac, Libbs, Pierre Fabre, Lilly, and Astra-Zeneca; travel grants from Roche/GNE and AstraZeneca; research grant to the institution from Roche/GNE, Astra-Zeneca, and GSK/Novartis. SDC reports being on the speaker’s bureau for AstraZeneca; and on the advisory board for Pierre-Fabre, IQVIA, and MEDSIR. All other authors have declared no conflicts of interest.
Figures
Similar articles
-
Association of Circulating Tumor DNA With Disease-Free Survival in Breast Cancer: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Nov 2;3(11):e2026921. doi: 10.1001/jamanetworkopen.2020.26921. JAMA Netw Open. 2020. PMID: 33211112 Free PMC article.
-
Role of circulating tumor DNA in early-stage triple-negative breast cancer: a systematic review and meta-analysis.Breast Cancer Res. 2025 Mar 12;27(1):38. doi: 10.1186/s13058-025-01986-y. Breast Cancer Res. 2025. PMID: 40075528 Free PMC article.
-
Association of Circulating Tumor DNA and Circulating Tumor Cells After Neoadjuvant Chemotherapy With Disease Recurrence in Patients With Triple-Negative Breast Cancer: Preplanned Secondary Analysis of the BRE12-158 Randomized Clinical Trial.JAMA Oncol. 2020 Sep 1;6(9):1410-1415. doi: 10.1001/jamaoncol.2020.2295. JAMA Oncol. 2020. PMID: 32644110 Free PMC article. Clinical Trial.
-
Circulating tumour DNA-Based molecular residual disease detection in resectable cancers: a systematic review and meta-analysis.EBioMedicine. 2024 May;103:105109. doi: 10.1016/j.ebiom.2024.105109. Epub 2024 Apr 13. EBioMedicine. 2024. PMID: 38614009 Free PMC article.
-
Association of post-operative ctDNA detection with outcomes of patients with early breast cancers.ESMO Open. 2024 Sep;9(9):103687. doi: 10.1016/j.esmoop.2024.103687. Epub 2024 Aug 30. ESMO Open. 2024. PMID: 39216186 Free PMC article.
Cited by
-
Peri-operative atezolizumab in early-stage triple-negative breast cancer: final results and ctDNA analyses from the randomized phase 3 IMpassion031 trial.Nat Med. 2025 Jul;31(7):2397-2404. doi: 10.1038/s41591-025-03725-4. Epub 2025 Jun 4. Nat Med. 2025. PMID: 40467898 Free PMC article. Clinical Trial.
-
Shifting the Paradigm: The Transformative Role of Neoadjuvant Therapy in Early Breast Cancer.Cancers (Basel). 2024 Sep 23;16(18):3236. doi: 10.3390/cancers16183236. Cancers (Basel). 2024. PMID: 39335206 Free PMC article. Review.
-
Liquid biopsy - a narrative review with an update on current US governmental clinical trials targeting immunotherapy.Future Sci OA. 2025 Dec;11(1):2527598. doi: 10.1080/20565623.2025.2527598. Epub 2025 Aug 7. Future Sci OA. 2025. PMID: 40772765 Free PMC article. Review.
-
The global progress and quality assessment of research on the association between circulating tumor DNA and clinical prognosis: a systematic review.J Natl Cancer Cent. 2024 Dec 27;5(2):156-166. doi: 10.1016/j.jncc.2024.10.002. eCollection 2025 Apr. J Natl Cancer Cent. 2024. PMID: 40265099 Free PMC article.
-
Circulating Tumor DNA in Early and Metastatic Breast Cance-Current Role and What Is Coming Next.Cancers (Basel). 2024 Nov 22;16(23):3919. doi: 10.3390/cancers16233919. Cancers (Basel). 2024. PMID: 39682108 Free PMC article. Review.
References
-
- Sung H., Ferlay J., Siegel R.L., et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. - PubMed
-
- Ignatiadis M., Sledge G.W., Jeffrey S.S. Liquid biopsy enters the clinic — implementation issues and future challenges. Nat Rev Clin Oncol. 2021;18(5):297–312. - PubMed
-
- Pascual J., Attard G., Bidard F.C., et al. ESMO recommendations on the use of circulating tumour DNA assays for patients with cancer: a report from the ESMO Precision Medicine Working Group. Ann Oncol Off J Eur Soc Med Oncol. 2022;33(8):750–768. - PubMed
-
- Burstein H.J., DeMichele A., Somerfield M.R., Henry N.L. Biomarker Testing and Endocrine and Targeted Therapy in Metastatic Breast Cancer Expert Panels. Testing for ESR1 mutations to guide therapy for hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer: ASCO guideline rapid recommendation update. J Clin Oncol Off J Am Soc Clin Oncol. 2023;41(18):3423–3425. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
