

Mortality reduction and cumulative excess incidence (CEI) in the prostate-specific antigen (PSA) screening era
- PMID: 38461151
- PMCID: PMC10925039
- DOI: 10.1038/s41598-024-55859-z
Mortality reduction and cumulative excess incidence (CEI) in the prostate-specific antigen (PSA) screening era
Abstract
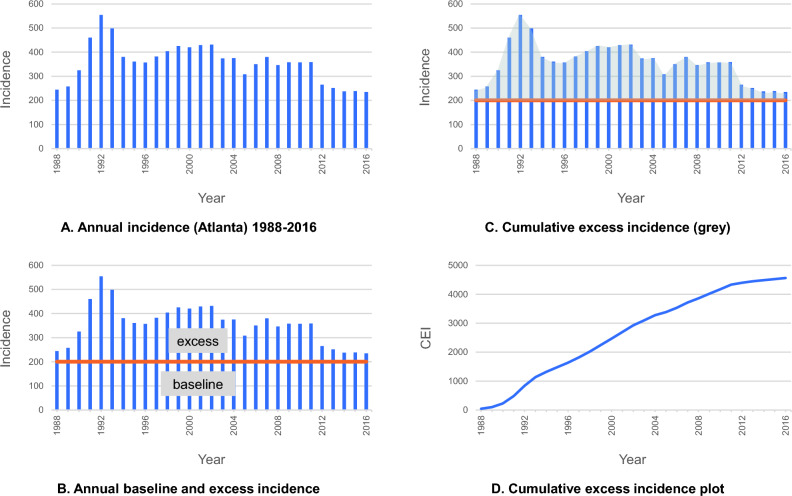
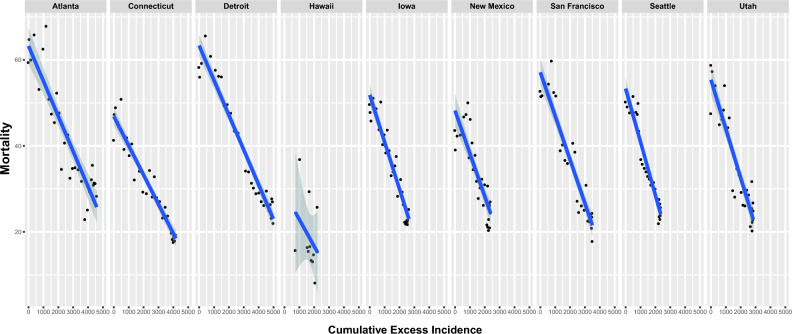
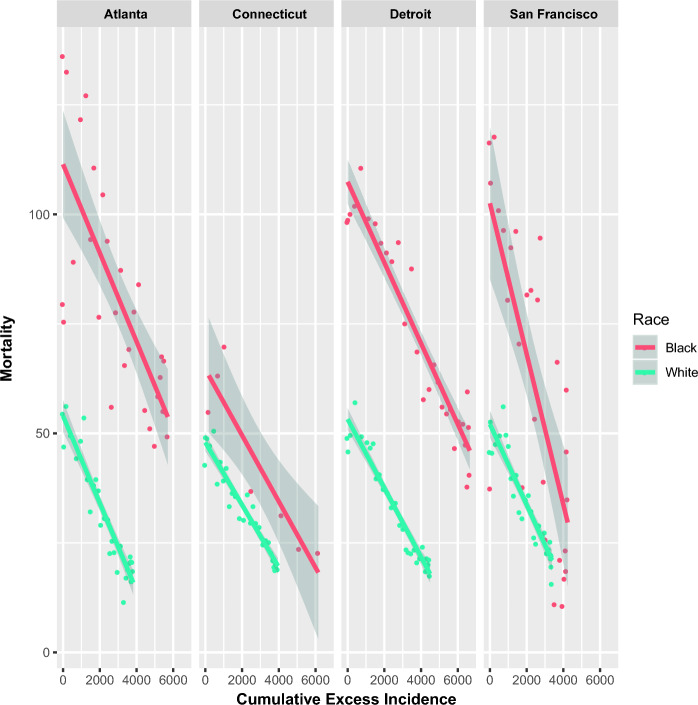
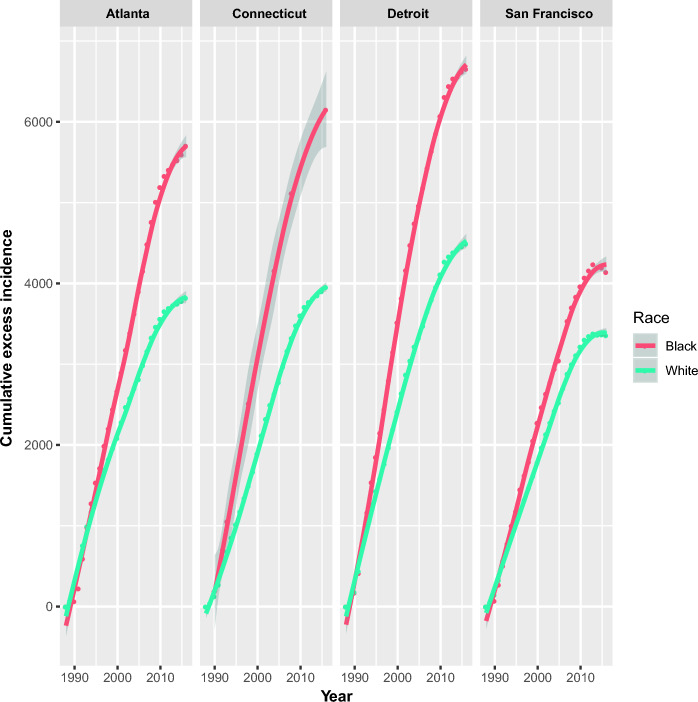
The extent to which PSA screening is related to prostate cancer mortality reduction in the United States (US) is controversial. US Surveillance, Epidemiology, and End Results Program (SEER) data from 1980 to 2016 were examined to assess the relationship between prostate cancer mortality and cumulative excess incidence (CEI) in the PSA screening era and to clarify the impact of race on this relationship. CEI was considered as a surrogate for the intensity of prostate cancer screening with PSA testing and subsequent biopsy as appropriate. Data from 163,982,733 person-years diagnosed with 544,058 prostate cancers (9 registries, 9% of US population) were examined. Strong inverse linear relationships were noted between CEI and prostate cancer mortality, and 317,356 prostate cancer deaths were avoided. Eight regions of the US demonstrated prostate cancer mortality reduction of 46.0-63.7%. On a per population basis, the lives of more black men than white men were saved in three of four registries with sufficient black populations for comparison. Factor(s) independent of CEI (potential effects of treatment advances) explained 14.6% of the mortality benefit (p-value = 0.3357) while there was a significant main effect of CEI (effect = -0.0064; CI: [-0.0088, -0.0040]; p-value < 0.0001). Therefore, there is a strong relationship between CEI and prostate cancer mortality reduction that was not related to factors independent of screening utilization. Minority populations have experienced large mortality reductions in the context of PSA mass utilization.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Opportunistic testing versus organized prostate-specific antigen screening: outcome after 18 years in the Göteborg randomized population-based prostate cancer screening trial.Eur Urol. 2015 Sep;68(3):354-60. doi: 10.1016/j.eururo.2014.12.006. Epub 2014 Dec 31. Eur Urol. 2015. PMID: 25556937 Clinical Trial.
-
Prostate cancer diagnosis and treatment after the introduction of prostate-specific antigen screening: 1986-2005.J Natl Cancer Inst. 2009 Oct 7;101(19):1325-9. doi: 10.1093/jnci/djp278. Epub 2009 Aug 31. J Natl Cancer Inst. 2009. PMID: 19720969 Free PMC article.
-
The Impact of Intensifying Prostate Cancer Screening in Black Men: A Model-Based Analysis.J Natl Cancer Inst. 2021 Oct 1;113(10):1336-1342. doi: 10.1093/jnci/djab072. J Natl Cancer Inst. 2021. PMID: 33963850 Free PMC article.
-
Population screening for prostate cancer and emerging concepts for young men.Clin Prostate Cancer. 2003 Sep;2(2):87-97. doi: 10.3816/cgc.2003.n.015. Clin Prostate Cancer. 2003. PMID: 15040869 Review.
-
Prostate cancer screening with prostate-specific antigen (PSA) test: a systematic review and meta-analysis.BMJ. 2018 Sep 5;362:k3519. doi: 10.1136/bmj.k3519. BMJ. 2018. PMID: 30185521 Free PMC article.
Cited by
-
Secondary Analysis of PSA and BCR-Free Survival in Asian Prostate Cancer Patients.Cancer Manag Res. 2025 Jun 24;17:1205-1214. doi: 10.2147/CMAR.S527092. eCollection 2025. Cancer Manag Res. 2025. PMID: 40584226 Free PMC article.
-
Small Area Estimation of PSA Testing in US States and Counties.Cancer Epidemiol Biomarkers Prev. 2025 Jan 9;34(1):197-204. doi: 10.1158/1055-9965.EPI-24-1086. Cancer Epidemiol Biomarkers Prev. 2025. PMID: 39513937 Free PMC article.
-
Prostate cancer temporal and regional trends in Brazil.Oncol Res. 2024 Sep 18;32(10):1565-1573. doi: 10.32604/or.2024.052179. eCollection 2024. Oncol Res. 2024. PMID: 39308515 Free PMC article.
-
The Effectiveness and Harms of PSA-Based Prostate Cancer Screening: A Systematic Review.Healthcare (Basel). 2025 Jun 9;13(12):1381. doi: 10.3390/healthcare13121381. Healthcare (Basel). 2025. PMID: 40565408 Free PMC article. Review.
-
Development and validation of a tool to assess the knowledge, awareness, and practice toward the screening of prostate cancer among adult men.J Educ Health Promot. 2025 May 30;14:211. doi: 10.4103/jehp.jehp_1093_24. eCollection 2025. J Educ Health Promot. 2025. PMID: 40575534 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
