

Two-stage palatal repair in non-syndromic CLP patients using anterior to posterior closure is associated with minimal need for secondary palatal surgery
- PMID: 38461271
- PMCID: PMC10924352
- DOI: 10.1186/s13005-024-00418-0
Two-stage palatal repair in non-syndromic CLP patients using anterior to posterior closure is associated with minimal need for secondary palatal surgery
Abstract
Objective: The aim of the present study was to assess the need for secondary palatal corrective surgery in a concept of palate repair that uses a protocol of anterior to posterior closure of primary palate, hard palate and soft palate.
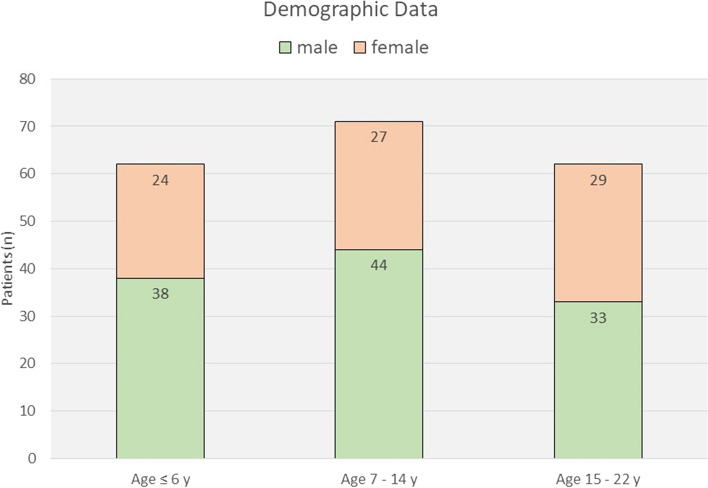
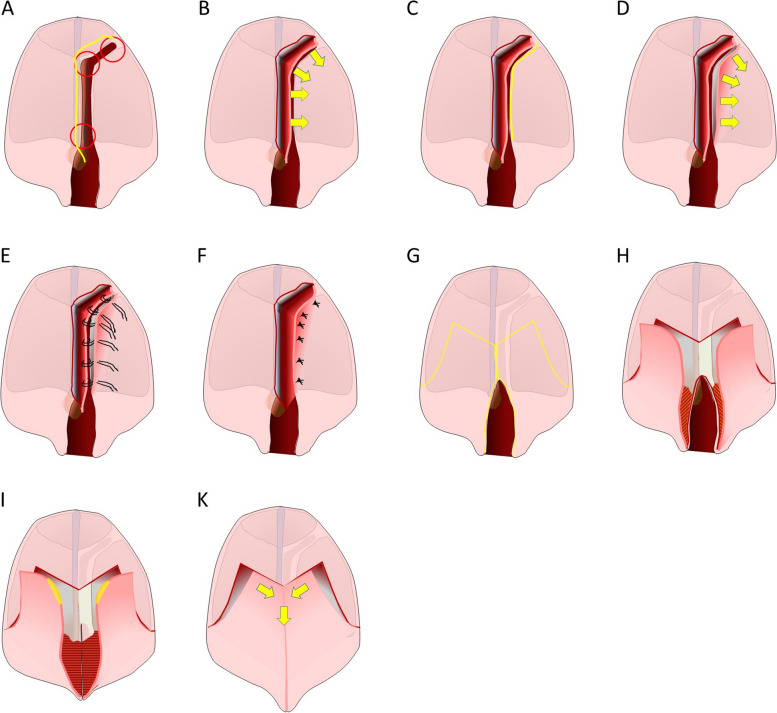
Methods: A data base of patients primarily operated between 2001 and 2021 at the Craniofacial and Cleft Care Center of the University Goettingen was evaluated. Cleft lips had been repaired using Tennison Randall and Veau-Cronin procedures in conjunction with alveolar cleft repair. Cleft palate repair in CLP patients was accomplished in two steps with repair of primary palate and hard palate first using vomer flaps at the age of 10-12 months and subsequent soft palate closure using Veau/two-flap procedures 3 months later. Isolated cleft palate repair was performed in a one-stage operation using Veau/two-flap procedures. Data on age, sex, type of cleft, date and type of surgery, occurrence and location of oronasal fistulae, date and type of secondary surgery performed for correction of oronasal fistula (ONF)and / or Velophyaryngeal Insufficiency (VPI) were extracted. The rate of skeletal corrective surgery was registered as a proxy for surgery induced facial growth disturbance.
Results: In the 195 patients with non-syndromic complete CLP evaluated, a total number of 446 operations had been performed for repair of alveolar cleft and cleft palate repair (Veau I through IV). In 1 patient (0,5%), an ONF occurred requiring secondary repair. Moreover, secondary surgery for correction of VPI was required in 1 patient (0,5%) resulting in an overall rate of 1% of secondary palatal surgery. Skeletal corrective surgery was indicated in 6 patients (19,3%) with complete CLP in the age group of 15 - 22 years (n = 31).
Conclusions: The presented data have shown that two-step sequential cleft palate closure of primary palate and hard palate first followed by soft palate closure has been associated with minimal rate of secondary corrective surgery for ONF and VPI at a relatively low need for surgical skeletal correction.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Alaluusua S, Hölttä E, Saarikko A, Geneid A, Leikola J, Heliövaara A. Speech symptoms of velopharyngeal insufficiency and the incidence of secondary speech surgery in 10-Year-old children with unilateral cleft lip and palate: comparison of 2 randomized surgical methods for primary palatal surgery. J Craniofac Surg. 2023;34(2):461–466. doi: 10.1097/SCS.0000000000008926. - DOI - PubMed
-
- Heliövaara A, Küseler A, Skaare P, Bellardie H, Mølsted K, Karsten A, et al. Scandcleft randomized trials of primary surgery for unilateral cleft lip and palate: comparison of dental arch relationships and dental indices at 5, 8, and 10 years. Eur J Orthod. 2022;44(3):258–267. doi: 10.1093/ejo/cjab055. - DOI - PMC - PubMed
-
- Küseler A, Mølsted K, Marcusson A, Heliövaara A, Karsten A, Bellardie H, et al. Scandcleft randomized trials of primary surgery for unilateral cleft lip and palate: maxillary growth at eight years of age. Eur J Orthod. 2020;42(1):24–29. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous