

Performance of a stool-based quantitative PCR assay for the diagnosis of tuberculosis in adolescents and adults: a multinational, prospective diagnostic accuracy study
- PMID: 38461830
- PMCID: PMC11142891
- DOI: 10.1016/S2666-5247(23)00391-9
Performance of a stool-based quantitative PCR assay for the diagnosis of tuberculosis in adolescents and adults: a multinational, prospective diagnostic accuracy study
Abstract
Background: Despite increasing availability of rapid molecular tests for the diagnosis of tuberculosis in high-burden settings, many people with tuberculosis are undiagnosed. Reliance on sputum as the primary specimen for tuberculosis diagnostics contributes to this diagnostic gap. We evaluated the diagnostic accuracy and additive yield of a novel stool quantitative PCR (qPCR) assay for the diagnosis of tuberculosis in three countries in Africa with high tuberculosis burdens.
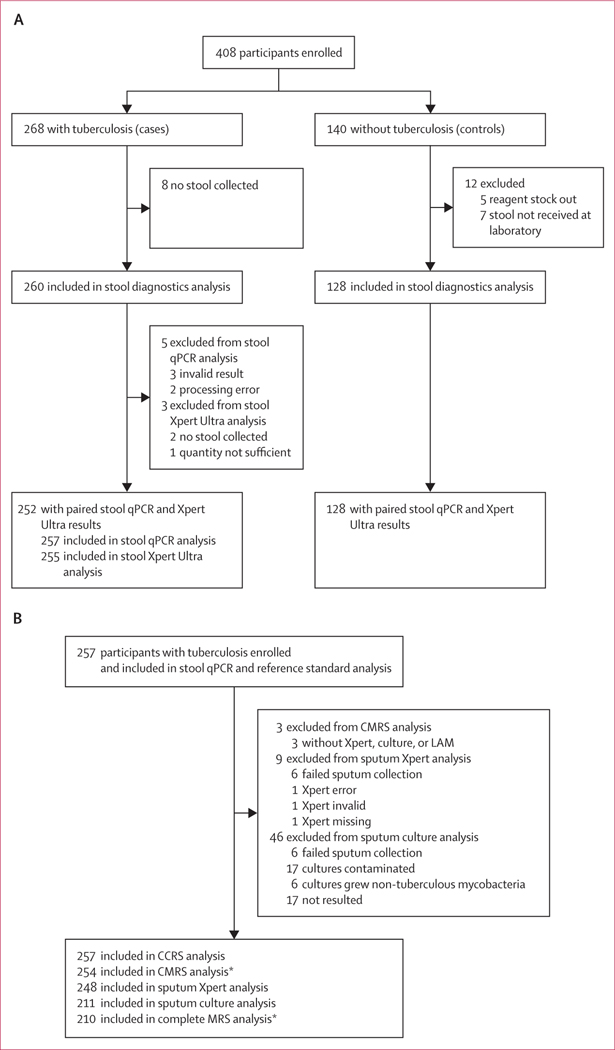
Methods: We undertook a prospective diagnostic accuracy study in Eswatini, Mozambique, and Tanzania from Sept 21, 2020, to Feb 2, 2023, to compare the diagnostic accuracy for tuberculosis of a novel stool qPCR test with the current diagnostic standard for Mycobacterium tuberculosis DNA detection from sputum and stool, Xpert-MTB/RIF Ultra (Xpert Ultra). Sputum, stool, and urine samples were provided by a cohort of participants, aged 10 years or older, diagnosed with tuberculosis. Participants with tuberculosis (cases) were enrolled within 72 h of treatment initiation for tuberculosis diagnosed clinically or following laboratory confirmation. Participants without tuberculosis (controls) consisted of household contacts of the cases who did not develop tuberculosis during a 6-month follow-up. The performance was compared with a robust composite microbiological reference standard (CMRS).
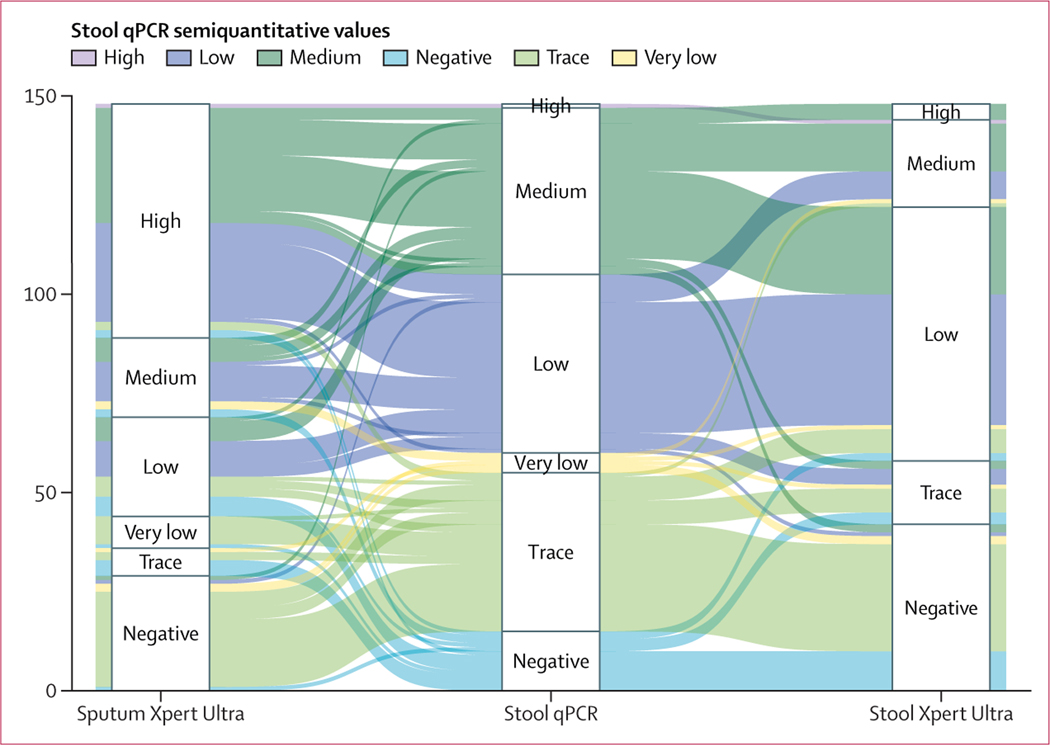
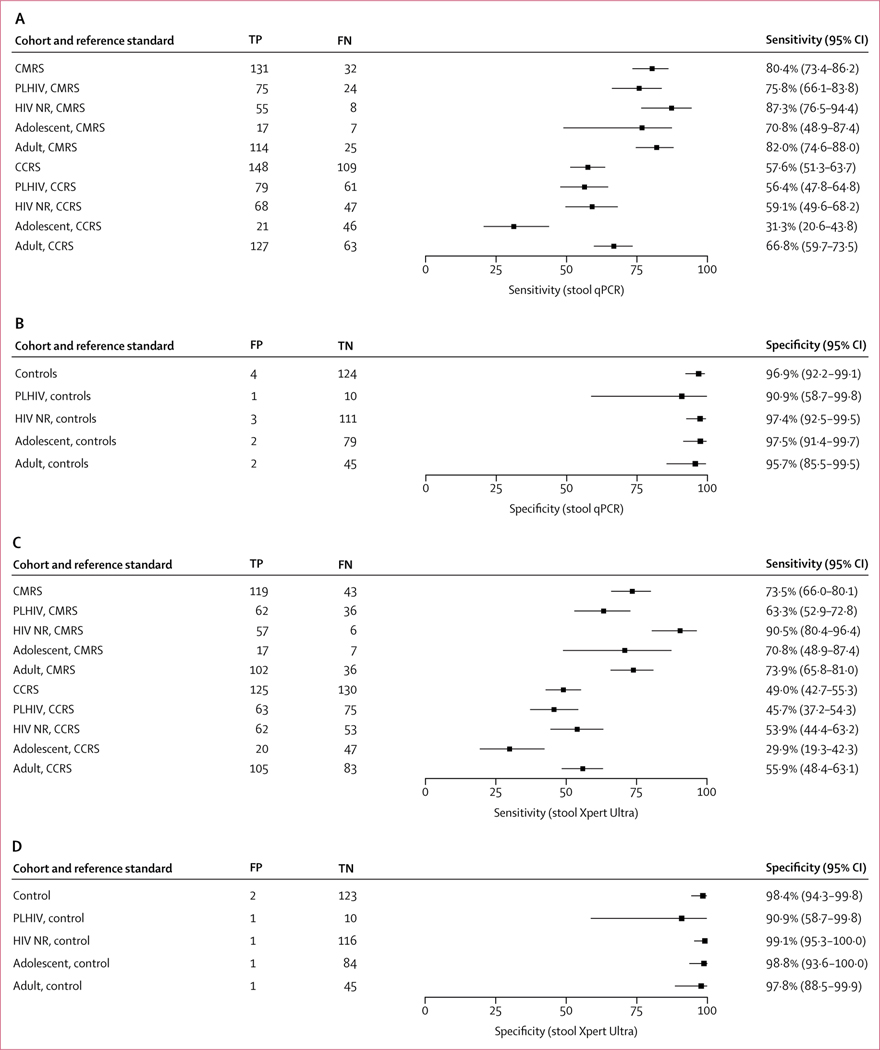
Findings: The cohort of adolescents and adults (n=408) included 268 participants with confirmed or clinical tuberculosis (cases), 147 (55%) of whom were living with HIV, and 140 participants (controls) without tuberculosis. The sensitivity of the novel stool qPCR was 93·7% (95% CI 87·4-97·4) compared with participants with detectable growth on M tuberculosis culture, and 88·1% (81·3-93·0) compared with sputum Xpert Ultra. The stool qPCR had an equivalent sensitivity as sputum Xpert Ultra (94·8%, 89·1-98·1) compared with culture. Compared with the CMRS, the sensitivity of the stool qPCR was higher than the current standard for tuberculosis diagnostics on stool, Xpert Ultra (80·4%, 73·4-86·2 vs 73·5%, 66·0-80·1; p=0·025 on paired comparison). The qPCR also identified 17-21% additional tuberculosis cases compared to sputum Xpert Ultra or sputum culture. In controls without tuberculosis, the specificity of the stool qPCR was 96·9% (92·2-99·1).
Interpretation: In this study, a novel qPCR for the diagnosis of tuberculosis from stool specimens had a higher accuracy in adolescents and adults than the current diagnostic PCR gold standard on stool, Xpert-MTB/RIF Ultra, and equivalent sensitivity to Xpert-MTB/RIF Ultra on sputum.
Funding: National Institutes of Health (NIH) Allergy and Infectious Diseases, and NIH Fogarty International Center.
Copyright © 2023 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests CL has received funding for this work from the German Center for Infection Research (DZIF); consulting fees from Insmed; and speakers' honoraria from Insmed, Gilead, GSK, and Janssen outside of the scope of this work. AMM has received honoraria from Janssen for participation in a data and safety monitoring board outside of the scope of this work. All other authors declare no competing interests.
Figures
References
-
- World Health Organization. Global tuberculosis report 2022. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/globa... (accessed Dec 13, 2022).
-
- Floyd K, Glaziou P, Zumla A, Raviglione M. The global tuberculosis epidemic and progress in care, prevention, and research: an overview in year 3 of the End TB era. Lancet Respir Med 2018; 6: 299–314. - PubMed
-
- World Health Organization. The End TB Strategy. 2015. https://www.who.int/tb/strategy/End_TB_Strategy.pdf?ua=1 (accessed Dec 13, 2022).
-
- World Health Organization. WHO consolidated guidelines on tuberculosis: module 3: diagnosis: rapid diagnostics for tuberculosis detection. 2020. https://apps.who.int/iris/bitstream/handle/10665/332862/9789240007307-en... (accessed Dec 13, 2022). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
