

Prescriptive and proscriptive lessons for managing shoulder dystocia: a technical and videographical tutorial
- PMID: 38462247
- PMCID: PMC10925798
- DOI: 10.1016/j.ajog.2022.03.016
Prescriptive and proscriptive lessons for managing shoulder dystocia: a technical and videographical tutorial
Abstract
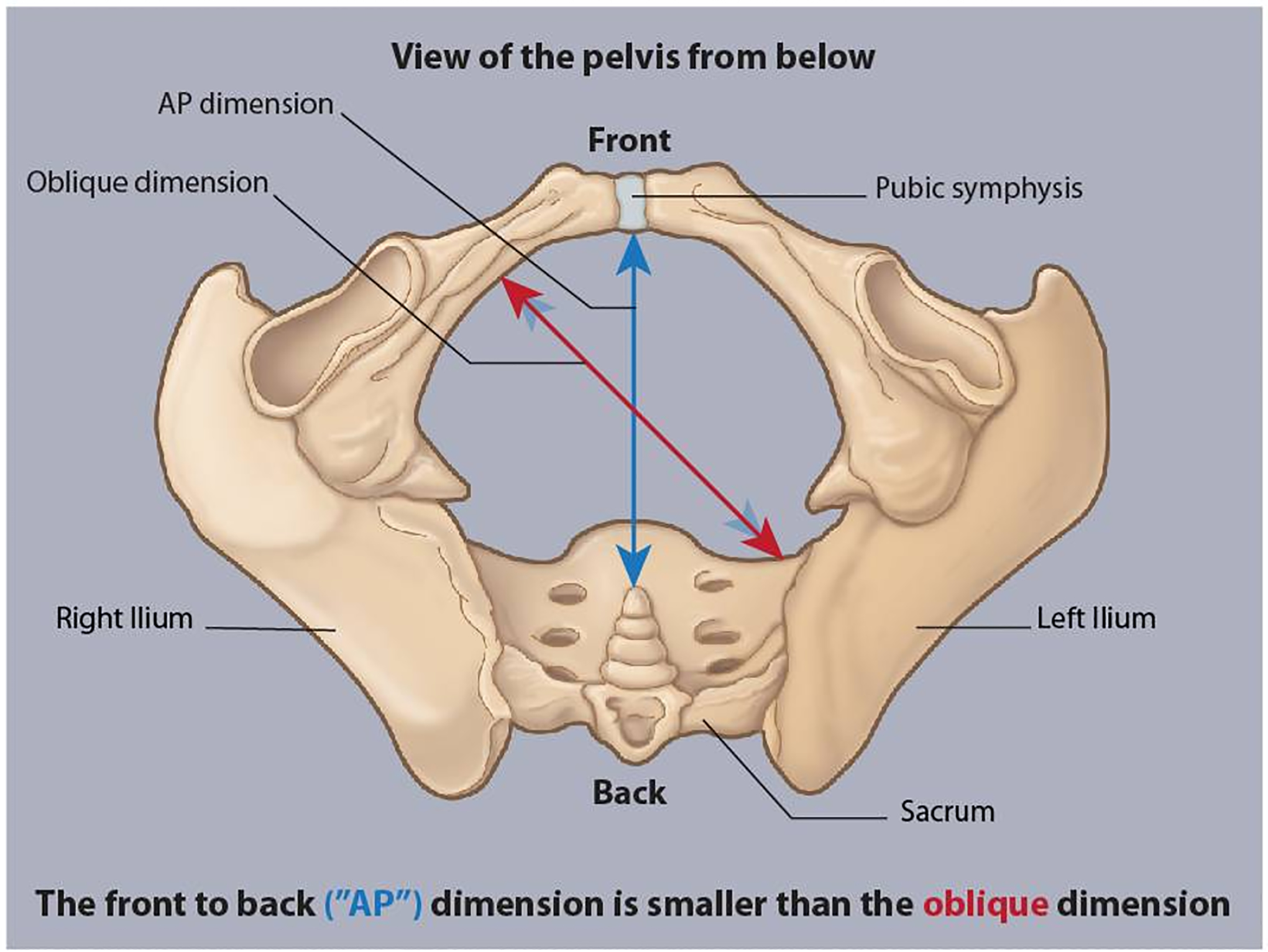
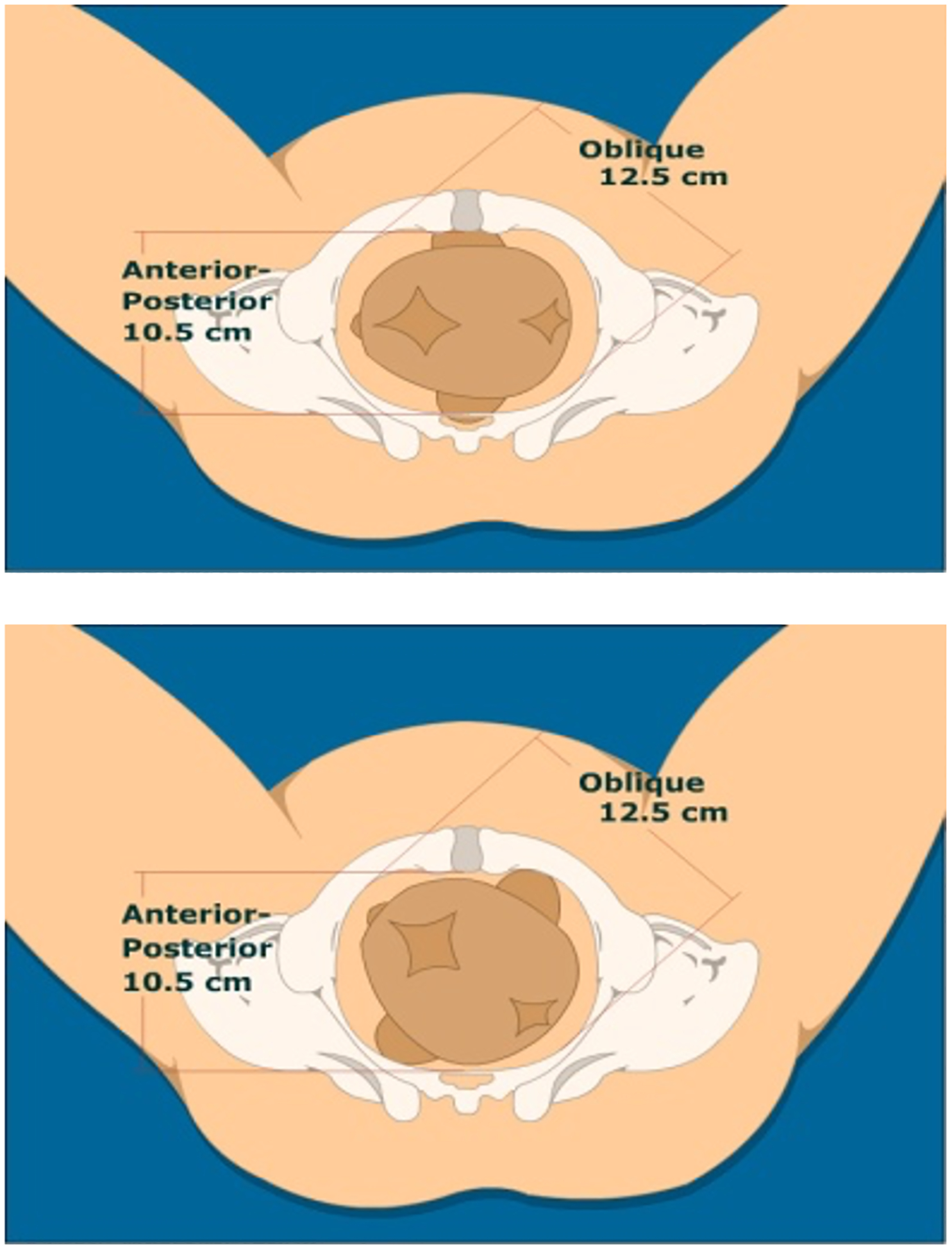
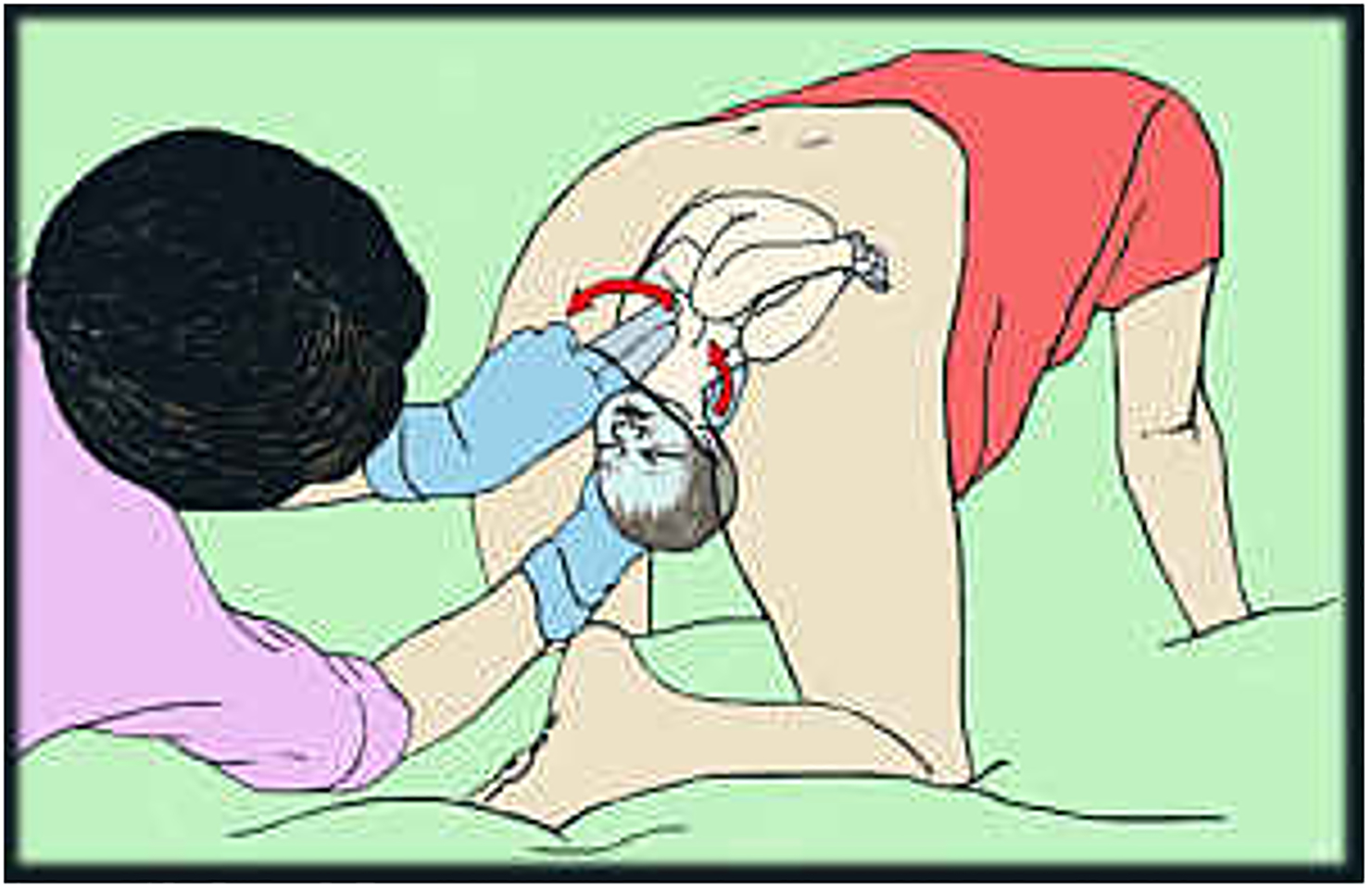
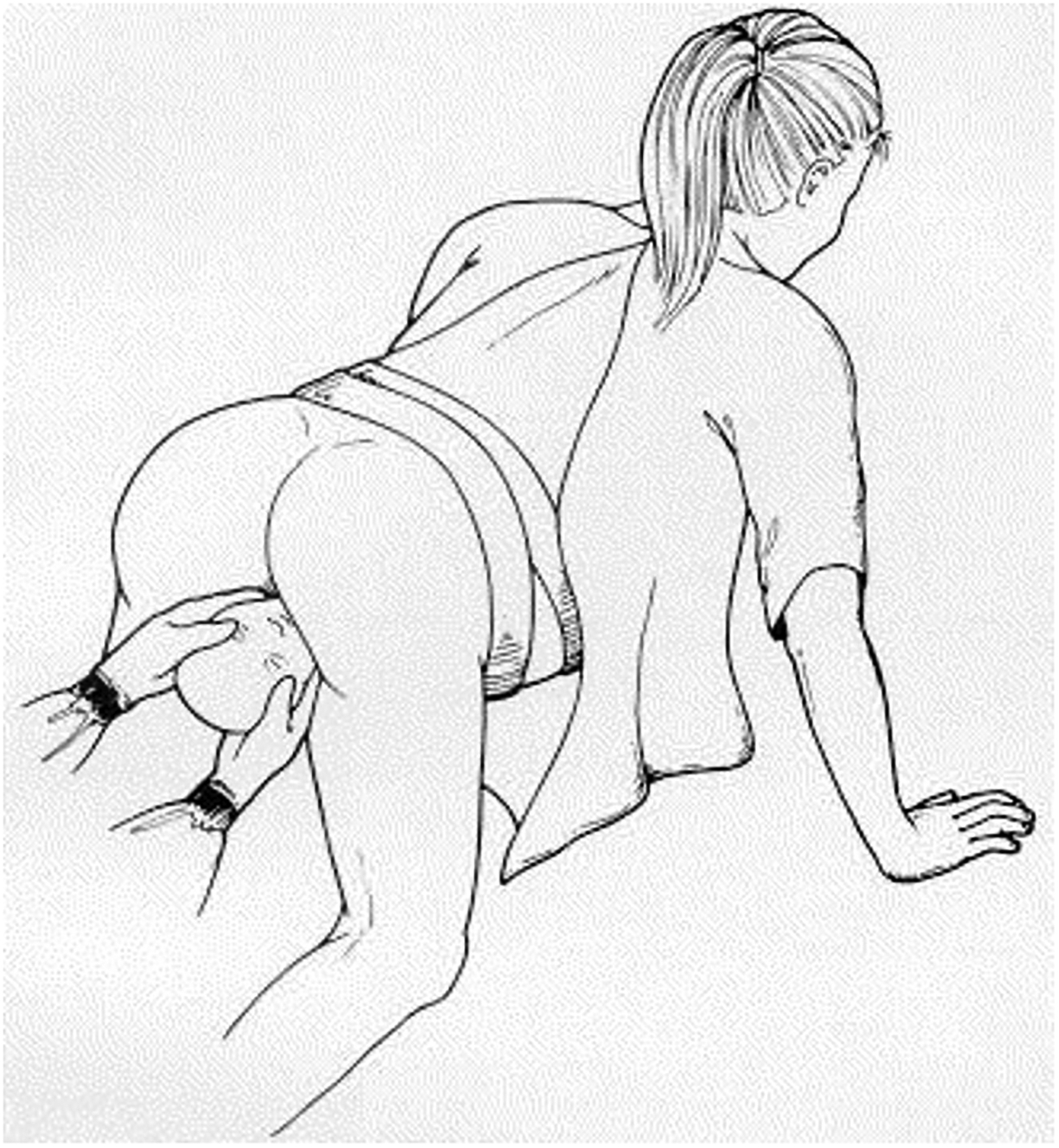
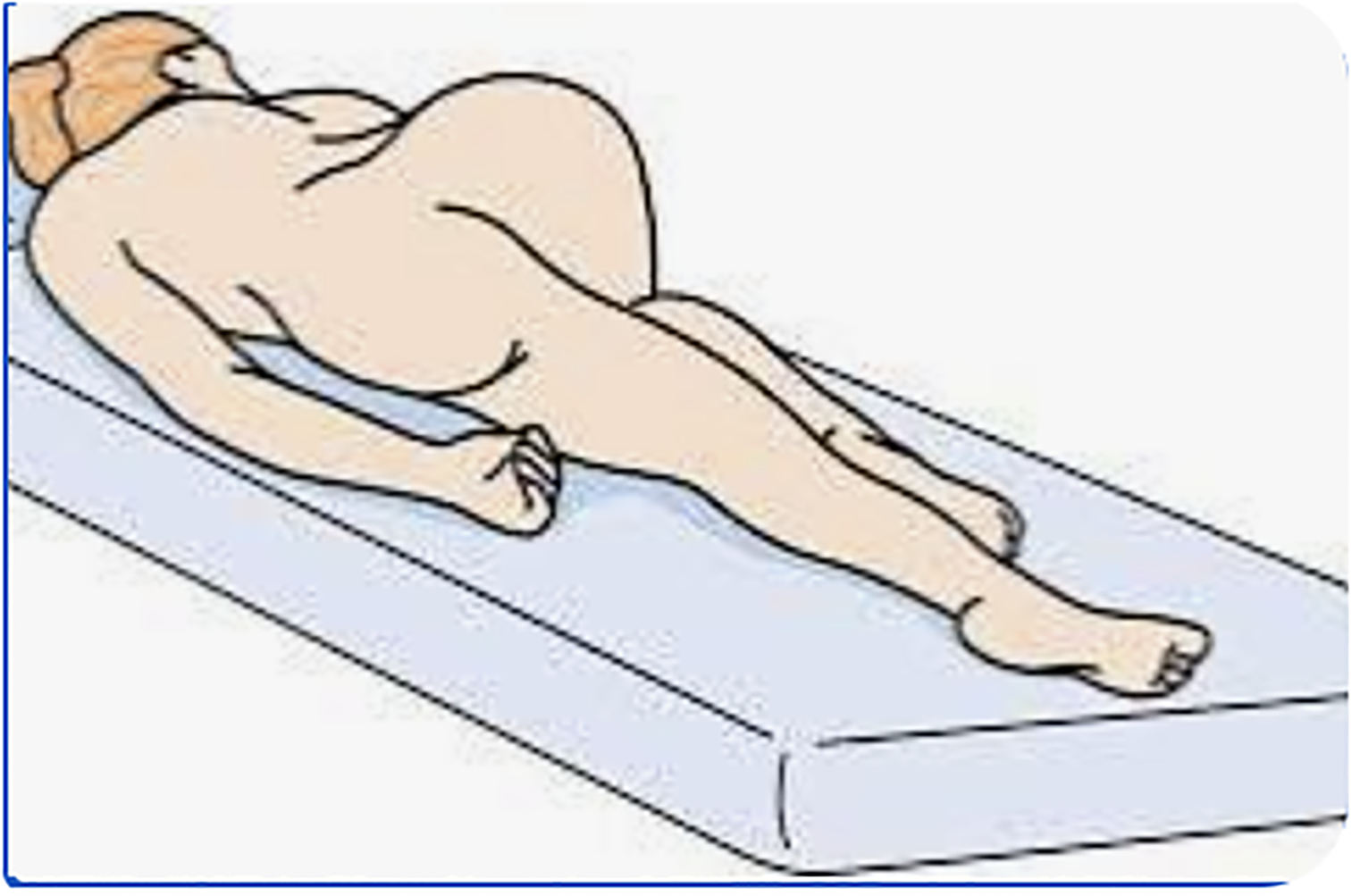
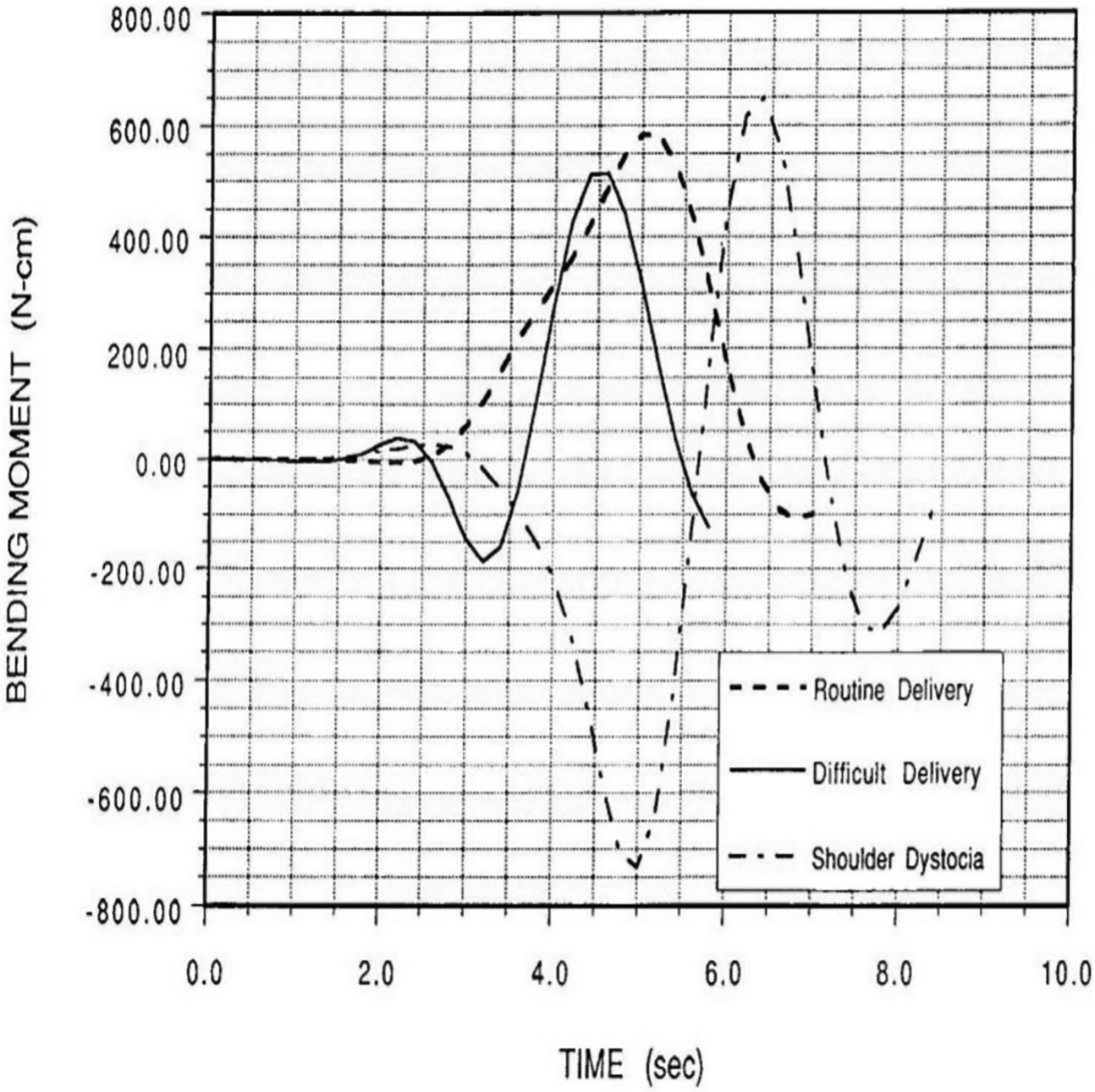
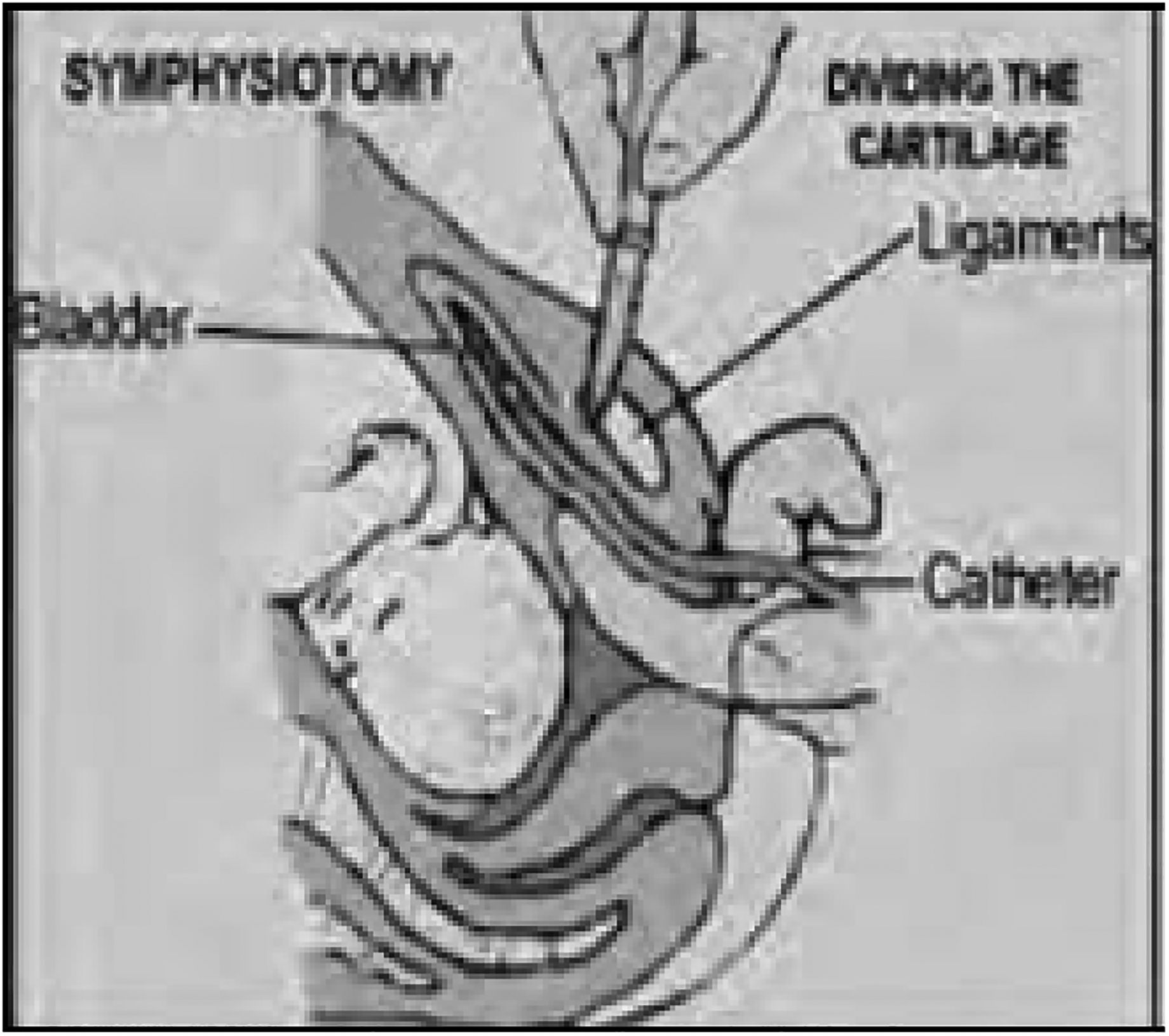
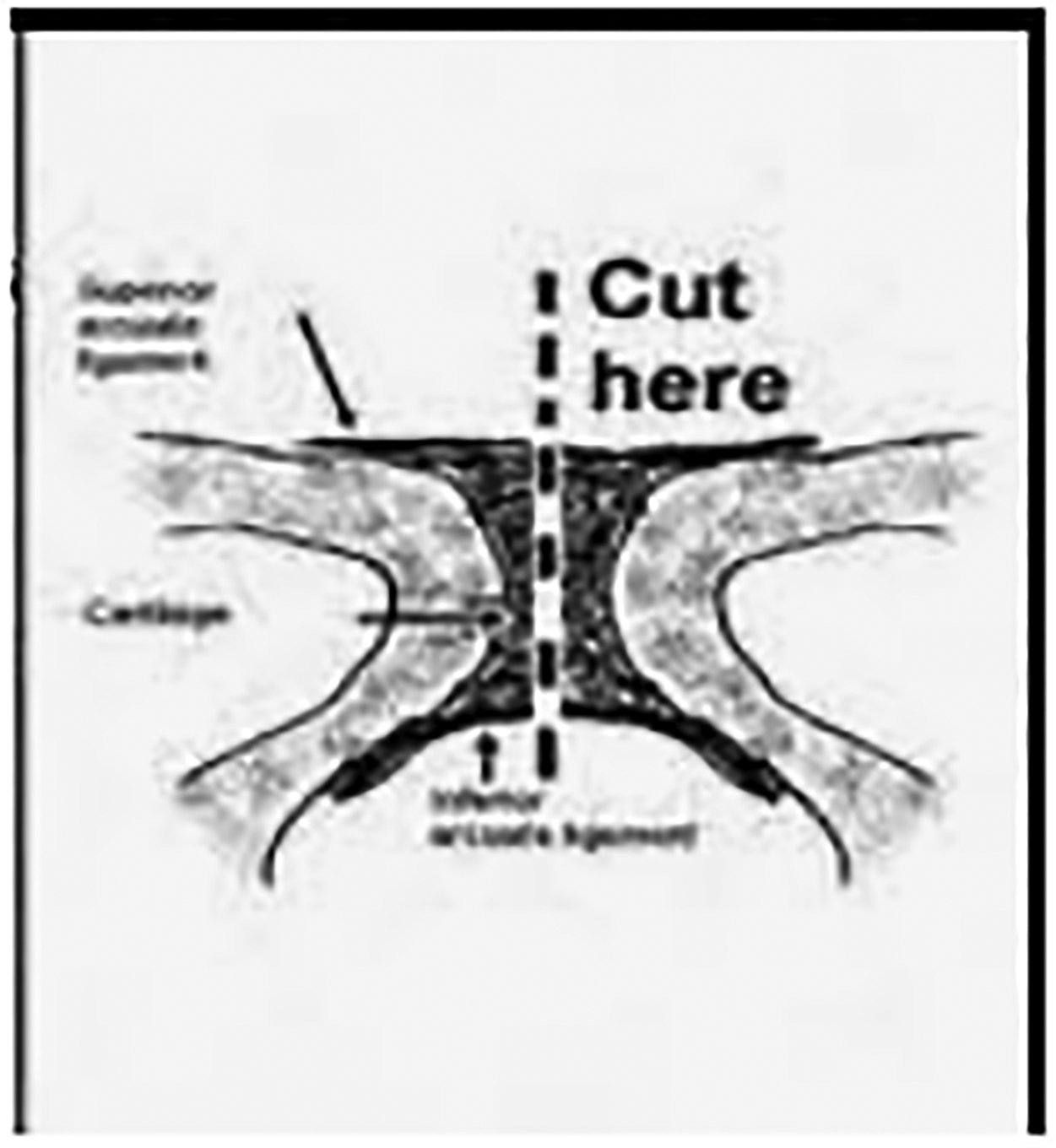
This tutorial of the intrapartum management of shoulder dystocia uses drawings and videos of simulated and actual deliveries to illustrate the biomechanical principles of specialized delivery maneuvers and examine missteps associated with brachial plexus injury. It is intended to complement haptic, mannequin-based simulation training. Demonstrative explication of each maneuver is accompanied by specific examples of what not to do. Positive (prescriptive) instruction prioritizes early use of direct fetal manipulation and stresses the importance of determining the alignment of the fetal shoulders by direct palpation, and that the biacromial width should be manually adjusted to an oblique orientation within the pelvis-before application of traction to the fetal head, the biacromial width is manually adjusted to an oblique orientation within the pelvis. Negative (proscriptive) instructions includes the following: to avoid more than usual and/or laterally directed traction, to use episiotomy only as a means to gain access to the posterior shoulder and arm, and to use a 2-step procedure in which a 60-second hands-off period ("do not do anything") is inserted between the emergence of the head and any initial attempts at downward traction to allow for spontaneous rotation of the fetal shoulders. The tutorial presents a stepwise approach focused on the delivering clinician's tasks while including the role of assistive techniques, including McRoberts, Gaskin, and Sims positioning, suprapubic pressure, and episiotomy. Video footage of actual deliveries involving shoulder dystocia and permanent brachial plexus injury demonstrates ambiguities in making the diagnosis of shoulder dystocia, risks of improper traction and torsion of the head, and overreliance on repeating maneuvers that prove initially unsuccessful.
Keywords: brachial plexus injury; maneuvers; negative instruction; positive instruction; simulation; visual didactics.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures



Similar articles
-
A critical evaluation of the external and internal maneuvers for resolution of shoulder dystocia.Am J Obstet Gynecol. 2024 Mar;230(3S):S1027-S1043. doi: 10.1016/j.ajog.2023.01.016. Epub 2023 Aug 17. Am J Obstet Gynecol. 2024. PMID: 37652778 Review.
-
Comparing McRoberts' and Rubin's maneuvers for initial management of shoulder dystocia: an objective evaluation.Am J Obstet Gynecol. 2005 Jan;192(1):153-60. doi: 10.1016/j.ajog.2004.05.055. Am J Obstet Gynecol. 2005. PMID: 15672018
-
[Shoulder dystocia: Guidelines for clinical practice--Short text].J Gynecol Obstet Biol Reprod (Paris). 2015 Dec;44(10):1303-10. doi: 10.1016/j.jgyn.2015.09.053. Epub 2015 Nov 2. J Gynecol Obstet Biol Reprod (Paris). 2015. PMID: 26541561 Review. French.
-
Shoulder dystocia: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF).Eur J Obstet Gynecol Reprod Biol. 2016 Aug;203:156-61. doi: 10.1016/j.ejogrb.2016.05.047. Epub 2016 May 30. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 27318182 Review.
-
Simulation of Shoulder Dystocia for Skill Acquisition and Competency Assessment: A Systematic Review and Gap Analysis.Simul Healthc. 2018 Aug;13(4):268-283. doi: 10.1097/SIH.0000000000000292. Simul Healthc. 2018. PMID: 29381590
Cited by
-
Video analysis of real-life shoulder dystocia to assess technical and non-technical performance.Acta Obstet Gynecol Scand. 2024 Oct;103(10):1985-1993. doi: 10.1111/aogs.14900. Epub 2024 Jun 24. Acta Obstet Gynecol Scand. 2024. PMID: 38925557 Free PMC article.
-
Shoulder Dystocia: A Comprehensive Literature Review on Diagnosis, Prevention, Complications, Prognosis, and Management.J Pers Med. 2024 May 30;14(6):586. doi: 10.3390/jpm14060586. J Pers Med. 2024. PMID: 38929807 Free PMC article. Review.
References
-
- Deering S, Poggi S, Macedonian C, Gherman R, Satin AJ. Improving resident competency in the management of shoulder dystocia with simulation training. Obstet Gynecol 2004;103(6);1224–1228. - PubMed
-
- Gurewitsch Allen ED. Simulation of shoulder dystocia for skill acquisition and competency assessment: a systematic review and gap analysis. Simul Healthc 2018;13(4):268–283. - PubMed
-
- Gonzalves A, Verhaeghe C, Bouet PE, Gillard P, Descamps P, Legendre G. Effect of the use of a video tutorial in addition to simulation in learning the maneuvers for shoulder dystocia. J Gynecol Obstet Hum Reprod 2018;47(4):151–155. - PubMed
-
- Kimmich N, Zimmermann R, Kreft M. Video analysis for the evaluation of vaginal birth: a prospective observational study. Swiss Med Wkly 2018;148:w14634. - PubMed
-
- Rosenberg K, Trevathan W. Birth, obstetrics and human evolution. Br J Obstet Gynaecol 2002;109(11):1199–1206. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
