

Exploration of potential immune mechanisms in cervical dystonia
- PMID: 38462403
- PMCID: PMC11162750
- DOI: 10.1016/j.parkreldis.2024.106036
Exploration of potential immune mechanisms in cervical dystonia
Abstract
Background: Although there are many possible causes for cervical dystonia (CD), a specific etiology cannot be identified in most cases. Prior studies have suggested a relationship between autoimmune disease and some cases of CD, pointing to possible immunological mechanisms.
Objective: The goal was to explore the potential role of multiple different immunological mechanisms in CD.
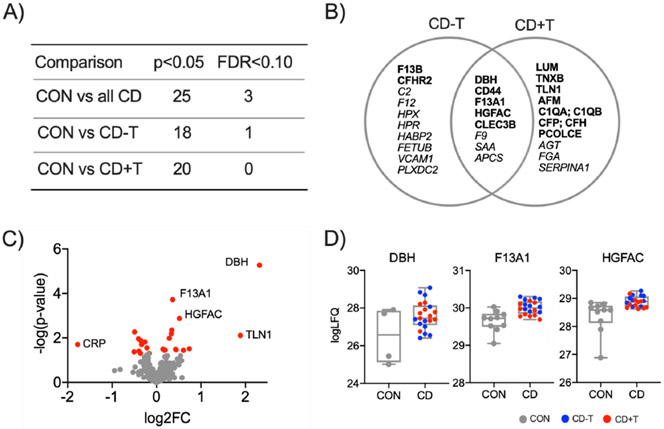
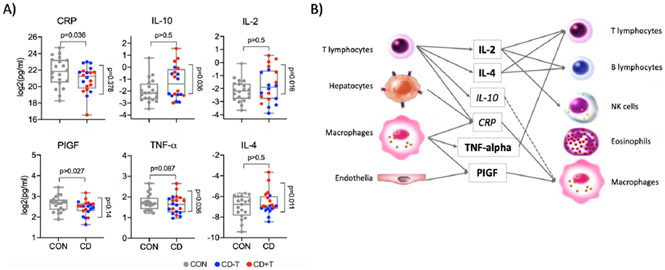
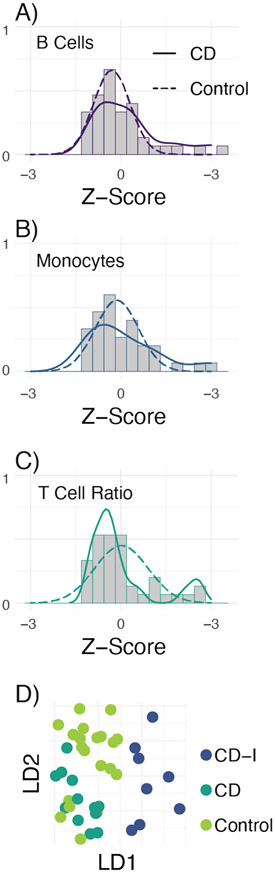
Methods: First, a broad screening test compared neuronal antibodies in controls and CD. Second, unbiased blood plasma proteomics provided a broad screen for potential biologic differences between controls and CD. Third, a multiplex immunoassay compared 37 markers associated with immunological processes in controls and CD. Fourth, relative immune cell frequencies were investigated in blood samples of controls and CD. Finally, sequencing studies investigated the association of HLA DQB1 and DRB1 alleles in controls versus CD.
Results: Screens for anti-neuronal antibodies did not reveal any obvious abnormalities. Plasma proteomics pointed towards certain abnormalities of immune mechanisms, and the multiplex assay pointed more specifically towards abnormalities in T lymphocytes. Abnormal immune cell frequencies were identified for some CD cases, and these cases clustered together as a potential subgroup. Studies of HLA alleles indicated a possible association between CD and DRB1*15:03, which is reported to mediate the penetrance of autoimmune disorders.
Conclusions: Altogether, the association of CD with multiple different blood-based immune measures point to abnormalities in cell-mediated immunity that may play a pathogenic role for a subgroup of individuals with CD.
Keywords: Autoimmune; Cervical dystonia; Dystonia.
Copyright © 2024. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of competing interest NO COI.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
